Download
1 / 78
780 likes | 790 Views
Basics in paediatric allergology: IgE-mediated allergy in respiratory illness. Prof. Dieter Koller, M.D. University Children´s Hospital of Vienna, Austria. Themes. Definition of allergy Overview on IgE-mediated allergies Methods in diagnosis

E N D
Basics in paediatric allergology: IgE-mediated allergy in respiratory illness Prof. Dieter Koller, M.D. University Children´s Hospital of Vienna, Austria
Themes • Definition of allergy • Overview on IgE-mediated allergies • Methods in diagnosis • Skin Prick testing, intradermal testing, atopy patch test, provocation testing • Allergy prevention • Primary, sekundary,tertiary prevention • Overview on studies dealing with prevention • Treatment • Symptomatic • causale (specific immuntherapy SCIT und SLIT) • Studies dealing with SCIT und SLIT
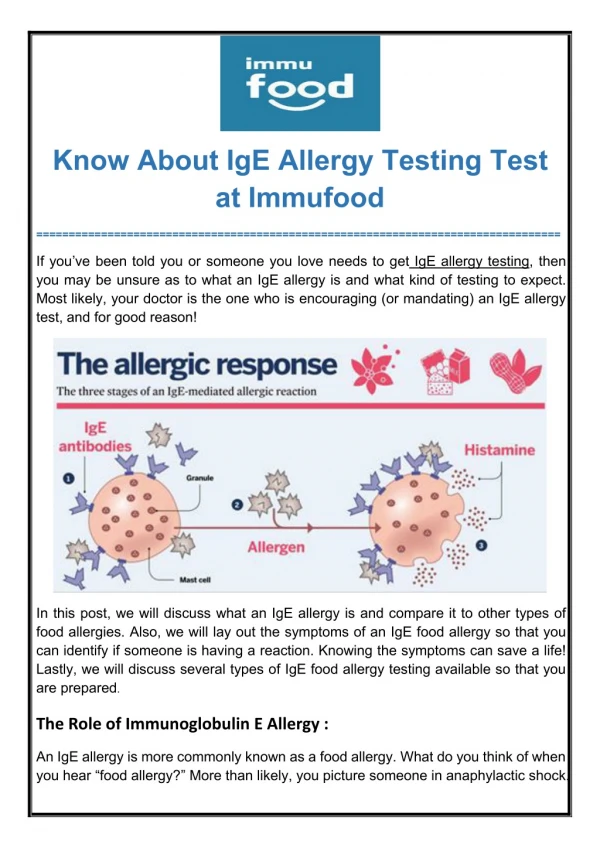
Allergic reaction • Manifestation of symptoms after repeated exposure to an allergen after (latent) period of sensitization • IgE-mediated release of mediators and zytokines from effector cells like mast cells, eosinophils and T-lymphocytes • Symptoms may occur in single organ but also systemically (allergic • Symptome zwar abhängig vom Zielorgan -systemisch allergische Reaktion jedoch immer möglich (z.B. allergische Rhinitis u. zeitgleiche Asthmasymptome)
Pseudoallergy and/or anaphylaktoid reactions • Symptoms similiar to allergic reaction –but not immunological mediated (Allergy tests negative)- and partially dependent on dosis • Histamine intolerance • Reaction auf radiocontrast agents,i.v. anaesthetics, antibiotics • Food adverse reactions to additives
Atopy:„a-topos“: “ being on the wrong place“ : ill-making reaction of the immune systeme Clemes von Pirquet (Head of the University Children´s Hospital Vienna1911-1929) defined the terminus Allergy/Atopy
Definition • Atopy: enhanced production of IgE in asymptomatic subjects • Allergy:Presence of symptoms corresponding to specific IgE antibodies
Manifestations of allergic diseases • Eyes - allergic conjunctivitis • Nose - allergic rhinitis • larynx- angioedema • Lung - allergic bronchial asthma • Skin – urticaria, rash • Gastrointestinal - diarrhea, abdominal cramps • Systemic - Anaphylaxis
Flow of systemic allergic reactions • Seconds to minutes after exposure of minimal amounts of allergen, sometimes after up to two hours • Biphasic reactions: rapide – improvement after treatment – further reaction • Prolonged reaction: Perstistence of symptoms under treatment
Allergic diseases • Bronchial asthma (extrinsic) • Allergic rhinoconjunctivitis (hay fever) • Atopic dermatitis • Food allergy • Insect sting allergy • Oral Allergy Syndrome (cross reactivity between pollens and certain fruits, like tree pollens and nuts, latex and banana, mango, house dust mite and snails, mussels, shrimps)
Prevalence of allergic diseases in the paediatric population • Atopic eczema: 10% • Allergic rhinoconjunctivitis: 10-20% • Bronchial asthma : 10% • Insect sting Allergy: 0.8 -1% • Food allergy: 3-4% • Anaphylaxis:1-4% • Drug allergy: ? (in 90% of children with positive history no detection of specific)
Genetics of allergic diseases • Until now, 79 genes have been identified to associated with the asthma and/or atopy phenotype in different populations. • Two major genes with association to the same phenotype independent of the population: • Arg 110Gln = variation of IL-13 (Th2-cytokine) encoded Gene is associated with increaseed IgE production • R510X = Gene variation causing lost of function of filagrin – atopic eczema
Diagnostic procedure Patients´ history in vivo, in vitro testing Provocation testing
Anamnesis • Which symptoms • Since when • When • How long • How frequent • Where • Which medication so far (improvement?)
Which symptoms may be associated with allergic diseases EczemaItching Erythema urticaria recurrentdiarrheaabdominal pain dystrophia Wheezingcoughing shortnessofbreath chronicstickynose sneezing recurrentrednessofeyesoritching
Diagnostics in allergy • In vivo (Skin-Prick testing,intradermal testing) • In vitro (spezific IgE, total IgE, tryptase …)
8 a old child; rhinoconjunctivitis since 2 years , end of May to middle of June
When are skin prick test false positive/negative? • Medication:antihistamines, steroids, immunosuppression • diseases:mastocytosis, atopiceczem, chronicurticaria, sunburn
Positive SPT result • negative = no wheal reaction, similar to the negative control • positive = wheal reaction of at least 3mm and equivalent to the histamine reaction.
Intradermal testing • Suspicion of hymenoptera allergy (drug allergy) • More sensitive than SPT but also more painful
In-vitro- testing • total IgE • specific IgE • ECP (eosinophil cationic protein) • tryptase
Total IgE: Indications • Indirect-diagnostic parameter if aspergillosis, parasitic infections, Job-syndrome • Detection of atopy(„nice to know but no need to know“) • Total IgE is no screening test (sensitivity <60%)
Primary indications for IgE measurement • Contraindicationsforskin prick testing • Diagnostics in infantsandtoddlers
Indication for using recombinant allergens (component) • ???? (notherapeuticconsequences) • Exception: hymenopteraallergy (Api m1, Ves v1, Ves v5) peanutallergy (Ara h2 – high riskforseverereactions)
In-Vitro-diagnostics- advantages - • Accurate and reproducable results • WHO controlled standards • Simple quantification (classes, Kilounits/l)
In-Vitro-diagnostics- disadvantages - • Measurement of circulating IgE-Ab, only • The level of antibodies does not correlate with clinical severity.
Provocation testing • Nasal • Conjunktivale • Bronchial • Oral • S.c. • i.v.
Nasal provocation testing • Especially with perennial allergens (mould, house dust mite) • Information about clinical relevance • Discrepancy between symptoms and SPT/IgE
conjunctival provocation testing • No screening test • Detection of allergic reactions of the eyes • Very sensitive, prove of allergy also when SPT or IgE negative • Einfach und meist risikolos
Bronchial provocation testing • Can a suspected allergen induce an asthma attack and in which dosage?
Conclusion! • In children with a positive family history for atopy an early sensitization against allergens is a significant risk factor for the development of brochial asthma.
Austrian Allergy Report 2006, T Dorner, A Rieder, K Lawrence,M Kunze,
Treatment of allergic diseases • Symptomatic:topical and/or systemic • antihistamines (H1-receptorblockers) • Dinatriumcromoglycate (nose, eye, lung) • topical steroids (nose, eye, lung, skin) • Causal: • Allergen avoidance if possible • Spezific immuntherapy – SIT
Allergic rhinitis and its impact on asthma ARIA Bousquet J et al. J Allergy Clin Immunol 2001 108 (5 Suppl): S 147-334