Download
1 / 30
300 likes | 595 Views
Perianal Crohn’s Disease. Dr. Bennet Rajmohan, MRCSEd, MRCS (Eng) Consultant General Surgeon. Case Presentation. History. 55 years / M Anal fistulectomy Mar 08, poor wound healing, faecal incontinence

E N D
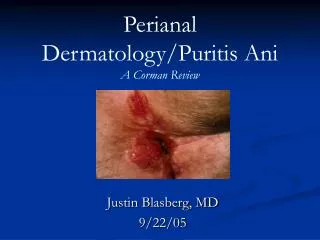
PerianalCrohn’s Disease Dr. Bennet Rajmohan, MRCSEd, MRCS (Eng) Consultant General Surgeon
History • 55 years / M • Anal fistulectomy Mar 08, poor wound healing, faecal incontinence • Admitted to Apollo – severe perineal & systemic sepsis Diverting loop transverse colostomy 25.03.08 • Occasional swelling & pus discharge from perineum • Colostomy closure planned • Diabetic for 3 years, currently on Insulin • No h/o HT or IHD
History • c/o faecal discharge from a hole near stoma – almost as much as normal quantity, instead of via stoma • Colostomy prolapse • Requested colostomy closure • Admitted in May ’09 • Colonoscopy followed by laparotomy planned
Diverting loop tranverse colostomy prolapse fistula
Perianal fistula fistulae
Colonoscopy Hepatic flexure pseudopolyps Rectum
Histopathology • Rectal biopsies Non specific proctitis, inflammatory cell infiltrate in lamina propria • Hepatic flexure biopsies Crohn’s colitis, Lamina propria with edema & dense inflammatory cell infiltration, mostly lymphocytes
Management • C-reactive protein – 96 mcg/ml, active inflammation • Medical Gastroenterology opinion • Surgery deferred • Hydrocortisone, steroid enemas, Mesalazine, Budesonide • Diabetic management • Symptoms improved, discharged on Mesacol, Budez • OP follow-up Improving, Infliximab therapy planned
Crohn’s disease • Occurs anywhere along GI tract from mouth to anus • Up to 90% of patients require at least one operation during their lifetime • Multiple recurrences, surgical excision not curative • Appropriate treatment of acute problem vs potential future exacerbations often a palliative procedure
Classification • 3 broad categories • Fistulizing • Fibrotic (stricturing) • Inflammatory • Fistula • Internal • External • Perianal • Enterocutaneous
Anorectal Crohn’s disease • Challenging aspect of Crohn’s • Overall up to 90% of patients • Isolated perianal disease in 10 to 15% • More common with concomitant proctitis or colitis
Diagnosis & evaluation • Direct observation of perineum – large skin tags, fissures or multiple fistulae hallmarks of Crohn’s • Digital rectal exam (DRE) & anoscopy • + Examination under anaesthesia (EUA) • Flexible or rigid sigmoidoscopy to evaluate rectum & sigmoid • Biopsies
Diagnosis & evaluation • EndoUltrasound (EUS) • Pelvic MRI • Examination Under Anaesthesia (EUA) • Diagnostic accuracy 85-90% each, 100% if 2 of above used together • Full GI tract evaluation • Colonoscopy & Upper GI scopy • Barium enema vs CT scan abdomen
Medical treatment • Therapy for anorectal Crohn’s similar to Intestinal Crohn’s • Antibiotics (Ciprofloxacin & Flagyl) – first-line agents • Avoid Steroids 9-fold increase in perianal abscesses • Aminosalicylates • Immunosuppressive medications 6-mercaptopurine & azathioprine, methotrexate, cyclosporin A
Medical treatment • Immunomodulators monoclonal anti-TNF antibodies (Infliximab) & azathioprine • Biologic therapies –TNF-binding neutralizing fusion proteins & interleukins • Other immunomodulators – thalidomide, tacrolimus & mycophenolate mofetil • Elemental diets, bowel rest with TPN, granulocyte- colony stimulating factor, hyperbaric O2 & Coagulation factor XIII
Infliximab • Crohn’s high levels of tissue TNF- α • Infliximab – IgG1 monoclonal antibody against TNF- α • 2 multicenter randomized, double-blind, placebo-controlled trials • IV infusion 5mg/kg at weeks 0, 2 & 6 • All fistulae closure – about 55% • About 11% developedperianal abscess • Enterocutaneous or peristomal fistulae not healed • Maintenance therapy needed, Expensive
Surgical treatment Anorectal abscess • Simple abscess I & D, close to anal verge – (potential future anal fistula) OR mushroom-tipped catheter (evacuate abscess & allow cavity to close around it) • Abscess with fistula – drainage & seton • Identify all foci of sepsis & provide adequate drainage • Avoid development of systemic symptoms, prevent local tissue destruction, thus preserving sphincter function
Anorectal fistula • American Gastroenterological Association (AGA) • Simple fistulae • Low (ie, below dentate line) superficial, low intersphincteric or low transsphincteric origin • Single external opening • No associated abscess • No rectovaginal fistula or anorectal stricture
Anorectal fistula • Complex fistulae • High in origin (high intersphincteric, high transsphincteric or suprasphincteric) • Multiple external openings • Associated abscess • Rectovaginal fistula or anorectal stricture • Distinction clinically important – • management varies • higher healing rates in simple fistulae
Surgery • Accurate diagnosis by EUA, pelvic MRI, anorectal EUS or all simple vs complex fistula • Presence or absence of active proctitis • Simple fistula, no proctitis • fistulotomy (90 – 100 % cure rate) • Alternatives – medical treatment, fistulotomy if antibiotics fail, endorectal advancement flap • Combined medical & surgical strategy – Infliximab with EUA & seton placement
Surgical treatment • Simple fistula with proctitis • poor fistulotomy wound healing • noncutting seton & medical therapy • Complex fistulae • combination medical & surgical therapy • seton drainage of abscesses, repair of rectovaginal fistulae & dilation of anorectal strictures • Infliximab plus an Immunomodulator
Seton placement before Infliximab • Higher initial response rate (near 100%) • Lower recurrence rate • Longer time to recurrence • 2 studies & 2 case series
Other considerations • Nutrition • Counselling • Incontinence • Previous sphincter damage • Scarring • Diarrhoea • Impaired rectal reservoir function resulting from longstanding proctitis
Severe perianal sepsis • D/D: tuberculosis, HIV, malignancy • Faecal diversion alone may heal perianal disease, at least temporarily • Not widely accepted, but potentially useful • Upto 80% symptom relief • Relapse with stoma in place occurs common • Stoma reversal rarely possible
Diverting stoma & bypass – Indications • Severe rectal & perianal fistula to resolve inflammation while trying to maximize medical therapy • Endorectal advancement flap (either concomitantly or before the procedure) • Septic patient with large terminal ileal-ascending colon phlegmon (difficulty identifying ureter etc) – resection & restoration of continuity later
Proctectomy • Needed in up to 25% of patients who have perianal disease And • Severe concomitant distal colonic & rectal involvement
Summary • Complex & unpredictable disease • Advances in medical therapy Management almost exclusively surgical to larger emphasis on medical therapy • Initial medical or combined Surgical & Medical • Surgery should focus on maximization of patient functional outcome & minimize complications