Download
1 / 54
540 likes | 718 Views
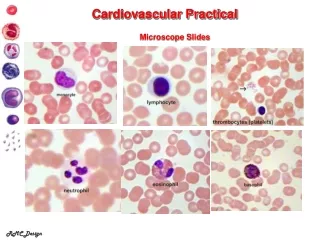
Cardiovascular practical Block. Shaesta Naseem Part I. 1-Atheroma of aorta. These three aortas demonstrate mild, moderate, and severe atherosclerosis from bottom to top. At the bottom, the mild atherosclerosis shows only scattered lipid plaques .

E N D
Cardiovascular practical Block ShaestaNaseem Part I
1-Atheroma of aorta These three aortas demonstrate mild, moderate, and severe atherosclerosis from bottom to top. At the bottom, the mild atherosclerosis shows only scattered lipid plaques. The aorta in the middle shows many more larger plaques. The severe atherosclerosis in the aorta at the top shows extensive ulceration in the plaques.
This is severe atherosclerosis of the aorta in which the atheromatous plaques have undergone ulceration.
CORONARY ATHEROSCLEROSIS • Partial occlusion of the artery lumen by an atheromatous plaque.
CORONARY ATHEROSCLEROSIS • The plaque consists of dissolved, cholesterol clefts, hyaline fibrous tissue and some blood capillaries.
Coronary atherosclerosis:Cross section of a coronary artery shows: • Partial occlusion of the lumen by an atheromatous plaque. • The plaque consists of dissolved, cholesterol clefts, hyaline fibrous tissue and some blood capillaries.
An example of an atherosclerotic aneurysm of the aorta in which a large swelling is seen just above the aortic bifurcation.
Aneurysmal dilatation of the lower aorta with evidence of rupture. There is an intraluminal thrombus with extensive aortic atherosclerosis .
The causes of aneurysms are: Advanced atherosclerosis (Usually abdominal aorta), Fungal infection (mycotic) Syphilis (thoracic aorta) Congenital (Berry aneurysm in circle of willis) .
Congested, hemorrhagic and soft area in the left ventricular wall Acute Myocardial infarction
Myocardial infarction • Cross section of the left and right ventricles shows a pale and irregular focal fibrosis and hemorrhagic/coagulative necrosis in the left ventricular wall with increased thickness . • Coagulative necrosis is the type of cell injury which usually occurs as a result of this lesion
MYOCARDIAL INFARCTION (LATE STAGE) • Chronic ischemic fibrous scar replacing dead myocardial fibers . The remaining myocardial fibers show enlarged nuclei due to ventricular hypertrophy .
Complications of MI: Arrhythmias, Ventricular rupture and hemopericardium Ventricular aneurysm Heart failure. Sudden death, Pericarditis The enzymes which are usually elevated in cases of MI CKMB, Troponin I and LDH
Heart from a hypertensive patient. • The left ventricle is very thick (over 2 cm). However the rest of the heart is fairly normal in size as is typical for hypertensive heart disease. • The hypertension creates a greater pressure load on the heart to induce the hypertrophy
In cross section, this view of the heart shows the left ventricle in the center left of the picture. • This heart is obtained from a severely hypertensive individual. • The left ventricle is grossly thickened. • The myocardial fibers have undergone hypertrophy.
Heart, normal Heart, left ventricular hypertrophy
6-Vegetations of rheumatic fever on mitral and aortic valves
Rheumatic valvulitis or Endocarditis The small verrucous vegetations seen along the closure line of this mitral valve are associated with acute rheumatic fever over areas of endocardial inflammation.
RHEUMATIC VALVULITIS (HEART) Irregular endocardial surface, no endocardial lining , focal fibrin deposits. The valve is thickened by dense hyalinized fibrous tissue with vascularization and chronic inflammatory cell infiltrate
Rheumatic valvulitis: Complications: • Valvularstenosis and regurgitation • Chronic rheumatic carditis • Heart failure • Thrombo-emboli secondary to atrial fibrillation • Subacuteendocarditis
Aschoff bodies /nodules • Aschoff bodies in the intermuscular fibrous septa. • They are oval in shape and seen in relation to blood vessels.
RHEUMATIC MYOCARDIITIS (ASHOFF NODULE) • Each consists of a focus of fibrinoid necrosis, few lymphocytes, macrophages and few small giant cells with one or several nuclei (Aschoff giant cell).
Acute rheumatic myocarditis:Section of cardiac muscle shows: • Aschoff bodies in the intermuscular fibrous septa. They are oval in shape and seen in relation to blood vessels. • Each consists of a focus of fibrinoid necrosis, few lymphocytes, macrophages and few small giant cells with one or several nuclei (Aschoff giant cell).
NUTMEG LIVER Section of liver showing alternating pale and dark areas with a nutmeg like appearance possibly due to passive congestion secondary to right sided heart failure.
The central portion of liver lobules shows congestion and dilatation of central veins and blood sinusoids, with atrophy and necrosis of liver cells.
Chronic venous congestion of the liver:Section of liver shows: • The central portion of liver lobules shows congestion and dilatation of central veins and blood sinusoids, with atrophy and necrosis of liver cells. • Kupffer cells contain few brown haemosiderin pigment granules.
The alveolar walls are thickened by dilated and engorged capillaries. • The alveoli contain edema fluid, red blood cells and heart failure cells.
Chronic venous congestion of the lung:Section of lung shows: • The alveolar walls are thickened by dilated and engorged capillaries. • The alveoli contain edema fluid, red blood cells and large alveolar macrophages (heart failure cells), which are filled with haemosiderin pigment derived from red cells breakdown. • In the late stage some fibrous tissue may also be seen.
10-Thromboangitis oblitrans (Buerger`s disease) This often leads to vascular insufficiency, and is characterized by segmental, thrombosingacute and chronic inflammation of medium and small sized artery. Especially tibia and radial artery involved.
Thromboangiitisobliterans (Buerger disease). The lumen is occluded by a thrombus containing abscesses (arrow), and the vessel wall is infiltrated with leukocytes.
Thromboagitis obliterans (Buerger’s disease):Section of the skin and subcutaneous tissue shows marked hyperkeratosis with inflammatory exudate in epidermis: • S mall blood vessels in the dermis show occlusive organized thrombi with recanalization and fibrosis around blood vessels. • Some blood vessels show recent organizing thrombi while others show infiltration of the wall and surrounding tissue by chronic inflammatory cells.
Giant cell arteritis • Prominent and tortuous and thickened scalp veins (temporal area) • Serous complication that might occur as a result of this disease include complete loss of vision and diplopia.
luminal stenosis Circumferential involvement of the vascular media is present (vertical arrow pointing downward). Also note the presence of chronic lymphocytic inflammation in the media and adventitia.
Giant cells can be of Langhans type or foreign-body type (three arrows) and may show fragments of disrupted internal elastic lamina
Giant cell (temporal) arteritis Fragmentation of internal elastic lamina, Giant cell reaction and Chronic inflammation
12-Leukocytoclastic / hypersensitivity vasculitis ( microscopic polyangitis )