Download
1 / 45
560 likes | 1.68k Views
THE PLEURA. GENERAL THORACIC SURGERY SECTION XI. ANATOMY OF THE PLEURA . EMBRYOLOGY Pleural cavity derivatives of primitive coelom—from splitting of the lateral mesoderm into splanchnic and somatic layers.

E N D
THE PLEURA GENERAL THORACIC SURGERY SECTION XI
ANATOMY OF THE PLEURA • EMBRYOLOGY • Pleural cavity derivatives of primitive coelom—from splitting of the lateral mesoderm into splanchnic and somatic layers. • The paired cavities separated by three partition into three subdivision: 1). Pericardial, 2). Pleural, 3). Peritoneal cavity. • The three partition are: 1). Unpaired septum transversum, 2) Paired pleuropericardial folds, 3) Paired pleuroperitoneal folds. • 4 weeks of development, laryngotracheal outgrowth from the floor of pharynx. • 5 week of development, two lung buds begin enlarge.
ANATOMY OF THE PLEURA • HISTOLOGY • The two layers of pleura have the similar histologic features. • The parietal pleura have stomata. • Each layer consists: 1) Innermost mesothelial cell layer, 2) Submesothelial interstitial connective tissue layer, 3) Inner thin elastic fiber layer, 4) Outer interstitial connective tissue layer, 5) Thick elastic fiber layer. 6) Another fatty layer separate the parietal pleura and the muscle of chest wall.
ANATOMY OF THE PLEURA • HISTOLOGY • The mesothelial cell vary in thickness, diameter, shape. The mesothelial cell demonstrate microvilli, tight apical junctions, the gap junction, desmosomes, half desmosomes. ( infrequently on the basal part of the cell menbrane) • In immunohistochemically, the mesothelial cell express low and high-molecular weight cytokeratin • Normal mesothelial cell are negative for reaction to vimentin, epithelial menbrane antigen, carcinoembryonic antigen, factor VIII-related antigen.
ANATOMY OF THE PLEURA • HISTOLOGY • Submesothelial layer contains collagen tissue, elastic fiber, small blood vesels, lymphatic network, nerve fiber. The cell in this layer is fibroblast, negative of cytokeratin, carcinoembryonic antigen, factor VIII-related antigen.
ANATOMY OF THE PLEURA • HISTOLOGY • Visceral and parietal pleura are the same thickness, 30-40μm. • The parietal pleura has large deiscences or stomata, 2-6μm, connect the pleural cavity with subpleural lymphstic network and permit egress of material into the lymphatics from the pleural space. • Focal accumulations of macrophages alone the pleuripotential mesenchymal lymphoid plasma cell in caudal portion of mediastinal pleura may functionally related to stomata.
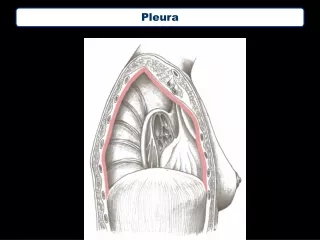
ANATOMY OF THE PLEURA • GROSS ANATOMY • Visceral pleura is closely applied to the lung surface, the cleavage plane is absence. • It line the major and minor fissure. The minor fissure may incomplete to absence in 50%. • The pulmonary ligment extend from hilar to diaphragm is consists of two apposed layer of visceral pleura and became continue with the parietal pleura.
ANATOMY OF THE PLEURA • GROSS ANATOMY • The parietal pleura lines the chest wall, mediastinum, diaphragm, and form the cupola or pleura dome at the thoracic inlet bilaterally. • The diaphragmatic pleura adheres tightly to the diaphragm. The mediastinum pleura adherent tightly to pericardium. The cupola, costal pleura can dissected from the underlying tissue. • The pleura recesses, usually two visible at chest PA, termed the 1) Azygoesophageal recess and the 2) Superior esophageal recess
ANATOMY OF THE PLEURA • BLOOD SUPPLY • Visceral pleura--- Artery supplied by bronchial and pulmonary arterial systems. The veins drain is pulmonary vein. • The parietal pleura--- Artery supply is from various systemic arterial supply the chest wall, diaphragm, and mediastinum.Vein is to the superior vena cava.
ANATOMY OF THE PLEURA • LYMPHATIC DRAINAGE • Subpleural space of the visceral pleura has large network of lymphatic channel but rarely subpleural lymph node. • The intrapulmonary lymph node incidence is 18%, nearly no node in subpleural space. • The lymphatic drainage of the visceral is to the pulmonary plexus located in interlobar and peribronchial space. The direct subplerual lymphatic connection to mediastinal node is 22-25%. • Subpleural connections were more in upper lobe than in lower lobes.
ANATOMY OF THE PLEURA • LYMPHATIC DRAINAGE • Lymphatic drainage of the parietal pleural is into the parietal pleural lymphatic channels, the stomata and Kampmeier’s foci play an important role. • The lymphatic network of the chest wall drain into internal mammary chain anteriorly and intercostals chain posteriorly. • The drainage of the diaphragmatic pleura is to retrosternal and mediastinal and celiac lymph node.
ANATOMY OF THE PLEURA • NERVE SUPPLY • Parietal pleura is innervated by both somatic and sympathetic and parasympathetic fiber via the intercostal nerve. • The diaphragmatic pleura is supplied by phrenic nerve. • The visceral pleura is devoid of somatic nerve.
RESORPTION OF GASES FROM THE PLEURAL SPACE 1. Normal condition: no free gases in the pleural space. 2. The virtual space between the parietal and visceral pleura is under negative pressure relation to atmosphere. 3. Normal condition: respiratory muscle in relaxtion state, the pressure is 5cm-H2O lower than surrounding atmosphere. The pressure decrease further during inspiration.( Especially the airwar obstruction, during Müller maneuver the pleural pressure can become negative to lower than 100 cm -H2O).
RESORPTION OF GASES FROM THE PLEURAL SPACE • FACTORS DETERMINING GAS RESORPTION • By a simple diffusion from the pleural space into the venous blood.this diffusion occurred in both directions. • No active transport mechanism for gas resoprtion. • The only driving forces that determine gas resorption are pressure gradients.
RESORPTION OF GASES FROM THE PLEURAL SPACE • The rate of gas resorption depends on four variables: • 1. Diffusion properties of gas. • 2. The pressure gradient for the gas in pleura in relation to venous blood. • 3. The area contact between pleura gas and pleura. • 4. Permeability of the pleural surface. • Ex: the oxygen is resorbed 62 times faster than nitrogen, CO2 23 times more soluable than O2. water and CO2 are equilibrate.
RESORPTION OF GASES FROM THE PLEURAL SPACE • PHASE OF GAS RESORPTION • Two phase in gas resorption. • Phase 1: equilibration of gases partial pressure. • Pahse 2: constant resorption.
RESORPTION OF GASES FROM THE PLEURAL SPACE • Three potential situation of pneumothorax result in different behavior of gas resorpion 1. Close rigid cavity: Non-reexpandable lung, could remain air filled. If the negative pressure is maintained fluid eventually seep into pleural cavity and gradually fills it, which subsequently solidifies and fibroses.
RESORPTION OF GASES FROM THE PLEURAL SPACE • 2. Closed collapsible cavity: The most frequent form of pneumothorax. It occurs when gas enter the pleural space, the opening responsible for pneumothorax becomes occluded, and lung are freely reexpabdable. As the gases resorbed no new gas enter the pleural space and the reexpansion of lungs compensates the volume, prevent the appearance of negative intrapleural pressure. It has been estimated that 6% of pneumothorax is absorbed in 24 hours.
RESORPTION OF GASES FROM THE PLEURAL SPACE • 3. Open cavity: the communication between the pleural cavity and the lung or through the thoracic wall persist the lung dosen’t reexpand.
RESORPTION OF GASES FROM THE PLEURAL SPACE • Different altitude in different barometric pressure. • Pneumothorax of 1-L volume would increase 33%if the patient was transported in an airplane pressurized at 8000 feet. • If a pneumothorax develop in deep sea 30 feet below the surface, the volume of pneumothorax would double as the diver resurfaces.
RESORPTION OF GASES FROM THE PLEURAL SPACE • THERAPEUTIC CONSIDERATION • 100% O2 is given to patient during a maneuver at high risk of creating pneumothorax (ex. transthoracic lung biopsy). • Reasons: • 1. The pneumothorax is filled with more soluble O2. • 2. the pressure greadient between pneumothorax and venous blood is larger because the 100% O2 washes out N2 from alveoli and eventually the venous blood. • The beneficial effect in relative small and not clinically useful.
PNEUMOTHORAX • ETIOLOGY • PRESENTATION • DIAGNOSIS • TREATMENT
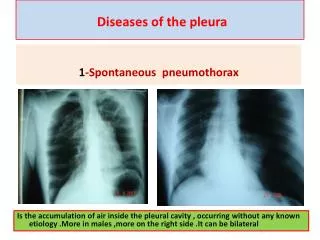
PNEUMOTHORAX • The most common cause of primary spontaneous pneumothorax is rupture of an apical subpleural bleb. • The etiology is obscure--- Difference in alveolar pressure in upright human between the base and the apex.
PNEUMOTHORAX • Spontaneous pneumothorax is rarely seen befor puberty. Children with spontaneous pneumothorax often have underlying disease such as cystic fibrosis. • More common in men (6:1). • More common in smoker. • Typical patient is young, tall, thin man in late adolescence and early adulthood.
PNEUMOTHORAX • PRESENTATION • Sudden onset chest pain, shortness of breath, not in engaging in any unusual or strenuous activity. • Spontaneous pneumomeiastinum is invariably associated with strenuous exertion such as bench-press weight lifting.
PNEUMOTHORAX • Special mention of secondary spontaneous pneumothorax associated with AIDS with Pneumocystitis pneumonia . • The most common sarcomna contributing to pneumothorax are osteosarcoma and synovial sarcoma.
PNEUMOTHORAX • Spontaneous rupture of esophagus present as pneumothorax without gastrointestinal symptoms. • Pneumothora accompanying pleural fluid, atelectasis. spontaneous pneumothorax with COPD especially with bullae formation is troublesome, tolerate poorly even small degree of collapse. • Catamenial pneumothorax, occurred first three days of menses, nonovulatory states such as pregnancy and oral contraceptive use were not associated with pneumothorax.
PNEUMOTHORAX • Lung cancer with pneumothorax only 0.03 to 0.05%. • Lymphangioleiomyomatosis seen in young women. • Acquired pneumothorax is most often iatrogenic, chest tube dysfunction. • Barotraumas pneumothorax is patient receving positive-pressure ventilation---treated by intervention rather than observation, indication for tube thoracostomy.
PNEUMOTHORAX • Tension pneumothorax: • Symptoms and sign: tachycardia, sweating, hypotention, mediastinal shift. • Clinical diagnosis of tension pneumothorax made on basis of appropriate history and physical findings is adequate to allow for emergency placement o chest tube without confirmatory chest radiography.
PNEUMOTHORAX • DIAGNOSIS: standard procedure is making chest x ray posteroanterior projection. • Should upright position, may miss a pneumothorax in semisupine portable anteroposterior view. • Lateral decubitus view if patient can’t be upright. • The percentage of collapse is underestimated. Artifact skin fold. • CT, cost effective.
PNEUMOTHORAX • Small fluid collections frequently encountered if pneumothorax over 24 hours. • The fluid always clear. • Large effusion often bloody and suggest a torn vascular adhesion, may require immediate operation to control bleeding.
PNEUMOTHORAX • Important to exclude a giant bullae in differential diagnosis because the tube drainage if such bullae is unrewarding. • Patient with pneumothorax should not be encouraged to travel by air.
PNEUMOTHORAX • 1.5% of the air is reabsorbed over each 24 hours. • Tube thoracostomy for pneumothorax over 30% or for patient with heart disease or COPD. • Tube place at anterior and mid-axillary line, less muscle tissue has to be traversed. • Anterior tube through second intercostal space, provide excellent apical air clearance but avoided in women.
PNEUMOTHORAX • The tube is placed by clump or trocar. • The trocar technique for its speed and convenience. • Pleur-evac drainage set to water-seal and gentle suction 20 cmh2op. • Routine suction may cause reexpansion pulmonary edema. • Chance of recurrence: 20-50%.
PNEUMOTHORAX • Various agents for induce pleural symphysis: siver nitrate, talc, hypertonic glucose, urea, oil, nitrogen mustard, various antibiotics. • Intrapleural tetracycline instillation could reduce the incidence of recurrence but difficulty to obtain. • Talc should be reserved for malignant effusion, not benign pneumothorax.
PNEUMOTHORAX • Open operation by limited lateral or axillary incision with bleb excision and pleural abrasion or limited apical pleurectomy--- excellent result, low recurrence. • Video-assisted thoracic surgery(VATS). • The recurrence rate is more high in VATS than other minithoracotomy.
PNEUMOTHORAX • Complete parietal pleurectomy should be reserved for open treatment failure, for postpneumonectomy patient with first pneumothorax and for old patient usually with COPD. • Bilateral pneumothorax could be treated for bilateral via median sternotomy.
PNEUMOTHORAX • Goal of surgical treatment is to find the offending bleb, remove it, encourage adhesion formation but not too dense an adhesion. • If no bleb is found, the apex of the upper lobe should be staple off.
PNEUMOTHORAX • Surgical treatment of AIDS patient: usually persistent air leak. • Thoracoscope approach with fibrin glue derivative. • YAG laser, Heimlich valves. • Persistent air leak who is poor operative risk,could be treated by using closed by pneumoperitoneum. • Conclusion: If surgical treatment is going to be necessary the sooner it is performed, the sooner that patient can resume a routine life style.