Download
1 / 60
1.3k likes | 4.35k Views
Atopic Dermatitis . Alyson W. Smith, MD Director of Pediatric Allergy St. Barnabas Hospital. Atopic dermatitis (AD) is a chronic, highly pruritic , eczematous skin disease that follows patients from early childhood into puberty and sometimes adulthood.

E N D
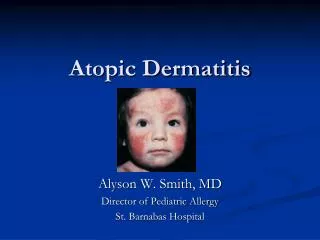
Atopic Dermatitis Alyson W. Smith, MD Director of Pediatric Allergy St. Barnabas Hospital
Atopic dermatitis (AD) is a chronic, highly pruritic, eczematous skin disease that follows patients from early childhood into puberty and sometimes adulthood. • Also referred to as eczematous dermatitis, the disease often has a remitting/flaring course, which may be exacerbated by social, environmental, and biological triggers.
Prevalence • Approximately 15% in the US and Europe • This represents a profound increase in recent years (from as low as 3% in 1960)
Natural History of Atopic Dermatitis • 60% of pts develop AD by 1 year of age. • 85% of pts develop AD by age 5. • Earlier onset often indicates a more severe course. • Many cases resolve by age 2, improvement by puberty is common. • 50%-60% of pts develop respiratory allergies or asthma. • 80% of occupational skin disease occur in atopics. • It is rare to see AD after age 50.
The Atopic March • Bergmann (1998, Clin Exp Allergy) Prospective birth cohort study, N 1314, 5yo If AD at 3 mos and one parent/sibling atopic >50% chance of asthma at age 5-6 • Castro-Rodriquez (1999, AJRCCM) Longitudinal, retrospective study, N 986 If AD and parental asthma; >75% chance of asthma during school years.
Filaggrin Filaggrins are filament-associated proteins which bind to keratin fibers in epithelial cells Individuals with truncation mutations in the gene coding for filaggrin are strongly predisposed to a severe form of dry skin, ichthyosisvulgaris, and/or eczema It has been shown that almost 50% of all severe cases of eczema may have at least one mutated filaggrin gene.
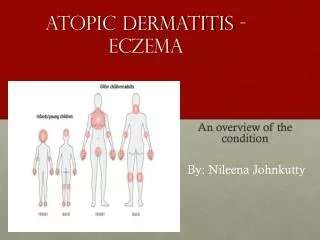
Infantile atopic dermatitis • Infants less than one year old often have widely distributed eczema. The skin is often dry, scaly and red with small scratch marks made by sharp baby nails. • The cheeks of infants are often the first place to be affected by eczema. • The diaper area is frequently spared due to the moisture retention of diapers. Just like other babies, they can develop irritant diaper dermatitis, if wet or soiled diapers are left on too long.
Toddlers and pre-schoolers • As children begin to move around, the eczema becomes more localized and thickened. Toddlers scratch vigorously and the eczema may look very raw and uncomfortable. • Eczema in this age group often affects the extensor (outer) aspects of joints, particularly the wrists, elbows, ankles and knees. It may also affect the genitals. • As the child becomes older the pattern frequently changes to involve the flexor surfaces of the same joints (the creases) with less extensor involvement. The affected skin often becomes lichenified i.e. dry and thickened from constant scratching and rubbing, • In some children the extensor pattern of eczema persists into later childhood.
Atopic dermatitis in school-age children • Older children tend to have the flexural pattern of eczema and it most often affects the elbow and knee creases. Other susceptible areas include the eyelids, earlobes, neck and scalp. • Many children develop a 'nummular' pattern of atopic dermatitis. This refers to small coin-like areas of eczema scattered over the body. These round patches of eczema are dry, red and itchy and may be mistaken for ringworm (a fungal infection). • Mostly the eczema improves during school years and it may completely clear up by the teens, although the barrier function of the skin is never entirely normal.
Food Allergy and Atopic Dermatitis • Children: • Moderate-Severe AD ( up to 33%) have (transient) clinically significant food allergy • Increasing severity of AD ~ increasing risk of food allergy • Adults: • Low incidence (<2%) • Foods responsible (~85% of cases): • Outgrown: Milk, egg, soy, wheat • Persistent: Peanut, nuts, fish, shellfish
Evaluation of Food Allergy in AD • Laboratory studies Specific IgE (Immunocap)-ONLY if clinically indicated! Skin prick testing Clinical evaluation: Elimination diets Oral food challenges Physician supervised Open, single blind, double-blind, placebo controlled
Triggers • Irritants Wool Soaps/detergents Disinfectants “Occupational” Tobacco smoke • Microbial agents Staph aureus Viral infection ?Dermatophytes • Heat/Sweating • Contactants • incl. Dust mites • Psychological • Foods(IgE-induced) vaso-dilatory items • Aeroallergens • Hormones • Climate
Managing AD(Preventative) • Prevent “scratching” or rubbing a) apply cold compresses to itchy skin • Carefully eliminate all the triggers of itch a) environmental, occupational, and temperature control b) bathing – soapless cleansers, Dove c) LUBRICATION – LUBRICATION LUBRICATION
Managing AD(Palliation) • Topical anti-inflammatory agents a) corticosteroids (ointments>creams) more potent - when “acute” least potent needed for “chronic” b) Tacrolimus 0.1% ointment, Pimecrolimus 1% Cream
Corticosteroids • These are the cornerstones of therapy of atopic dermatitis. The following principles should be adhered to while instituting topical steroid therapy: • High potency steroids are used for a short period to rapidly reduce inflammation. • Maintenance therapy, if needed is best done with mild steroids like hydrocortisone. • On face and intertriginous areas, mild steroids should be used, mid-potency formulations are used for trunk and limbs.
Corticosteroids • Topical steroids are applied initially twice or three times a day. After the symptoms are lessened, frequency of application should be reduced. Intermittent use if topical steroid may be alternated with application of emollients. • Ointments are superior to creams or lotions. • The potential side-effects of topical steroids should always be kept in mind. • Systemic steroids: a short course of systemic steroids (prednisolone, triamcinolone) may occasionally be needed to suppress acute flare-ups. • Intralesional steroids (triamcinoloneacetonide) may help resolve thickened plaques of eczema not responding to topical agents
Calcineuron InhibitorsIndications • Protopic (tacrolimus) Ointment, both 0.03% and 0.1% for adults; 0.03% for children aged 2-15 years • For short-term and intermittent long-term therapy in the treatment of moderate to severe atopic dermatitis in patients • For whom the use of alternative, conventional therapies are deemed inadvisable because of potential risks or • Who are not adequately responsive to, or are intolerant of alternative, conventional therapies. • Elidel (Pimecrolimus Cream 1%) for patients 2 years of age and older • For short-term and intermittent long-term therapy in the treatment of mild to moderate atopic dermatitis in non-immunocompromised patients • For whom the use of alternative, conventional therapies are deemed inadvisable because of potential risks or • Who are not adequately responsive to, or are intolerant of alternative, conventional therapies.
Calcineuron Inhibitors Advantages • A Rx option to CS • No steroid atrophy • For adults and child- ren >2yrs. • Sx improvement within 1-3 weeks. • Long-term intermittent use • Limitations • Off-label for children <2 yrs. • Burning, stinging, itching, after application – often minimal and transient. • Black box warning
Basis for FDA concern • Because of a perception by physicians and patients that topical pimecrolimus and tacrolimus are safer than steroid preparations, they had been increasingly been used as first-line therapy and off label. There were almost 2 million prescriptions written of these topical medications for children between June 2003 and May 2004 and approximately half a million were for those under 2 years of age. • Known toxicity of immunosuppressant doses of systemically administered tacrolimus: lymphoproliferative disease, photocarcinogenicity, and increased risk of nonmelanoma skin cancers • Animal studies in mice, rats, and monkeys have found an increased risk of lymphoma and skin cancers with topical and oral exposure to calcineurin inhibitors (dose used 30x maximum human dose in monkey study) • March 2010-46 cancer cases and 71 infection cases have been reported in patients aged 16 and younger from 2004 to 2008 with Novartis' Elidel and Astellas' Protopic.
More controlled studies are needed on the use of TCI, especially in patients less than two years. • Long term effects not known. • Should only be used as a second line agent.
Emollients Atopic dermatitis patients frequently have dry skin which is aggravated during winter months. Xerosis (dryness) breaks the barrier function of the skin and promotes infection and inflammation. Ointments are preferred over lotions or creams. Emollients should be applied immediately after a soaking bath to retain the moisture. Emollients containing urea or alpha-hydroxy acids often cause stinging or burning sensations.
Antihistamines • Antihistamines give variable results in controlling pruritus of atopic dermatitis since histamine is not the only mediator of itching in atopic patients. • Any of the non-sedating antihistamines like cetirizine, loratadine or fexofenadine may be used. • The conventional antihistamines like diphenhydramine or hydroxyzine may give better results for their additional actions as a sedative or anxiolytic. • Topical antihistamines should be avoided for their sensitizing potential.
Antimicrobials Infections and colonization with Staphylococcus aureus may aggravate or complicate AD. Antibiotics like erythromycin, cephalosporins, or cloxacillin are usually prescribed. Dermatophytosis or Pityrosporum infections are treated with antifungals. Acyclovir or other appropriate antiviral agents should be promptly advised for treatment of herpes simplex infections.
Oral immunomodulators • Cyclosporine: By virtue of its immunomodulating action, cyclosporine has a limited role in controlling atopic dermatitis in recalcitrant adult cases. The potential side effects should always be kept in mind. • Azathioprine: This immunosuppressive agent has also been used in severe adult cases. Again, potential side effects limit its role in selected cases.
Other Therapies Tar may be useful, particularly for the scalp, over the counter, smelly, stained clothes Phototherapy Ultraviolet B (UVB) alone, or in combinations with UVA may be beneficial in selected patients. Probiotics The rationale for their use is that bacterial products may induce an immune response of the TH 1 series instead of TH 2 and could therefore inhibit the development of allergic IgE antibody production. Chinese herbal medicine Some Chinese herbal preparations contain prescription medications, including prednisone, and have been associated with cardiac and liver problems. Bleach baths-A randomized, investigator-blinded, placebo-controlled trial including 31 patients showed that intranasal mupirocin ointment and diluted bleach (sodium hypochlorite) baths improved atopic dermatitis symptoms in patients with clinical signs of secondary bacterial infection.
Complications of AD • Secondary Infection a) bacterial impetiginization “super-antigenicity” b) viral localized – verruca, molluscum, herpes systemic – Kaposi’s herpetiform eruption c) mycotic Dermatophyte Candidal
Staphylococcus aureus & Skin • S. aureus–a saprophytic bacteria detected in 5% to 30% of healthy persons skin and in 20% of their nares. • S. aureus – carriage rate in AD is 76% for uninvolved skin, 93% for lesional skin and 79% for the anterior nares. • S. aureuscolonizationhas potential to modify dermatologic diseases, in particular, S. aureusenterotoxins A-E – can act as “superantigens”. • Superantigens bind as intact proteins to T-cell receptors and MHC class II molecules.
HSV- ezcema herpeticum • Clusters of multiple, uniform, 2-3mm crusted papules and vesicles develop in untreated or poorly controlled atopic dermatitis. The initial infection may be accompanied by fever, malaise, and lymphadenopathy. • Complications: keratoconjunctivitis and viremia (multiple organ involvement with meningitis and encephalitis) • Tx: acyclovir (PO for mild, localized symptoms), hospitalization for febrile, ill-appearing or young infants, No steroids or calcineurin inhibitors
Differential Diagnosis of Atopic Dermatitis • Dermatitis -Contact -Seborrheic • Immunodeficiencies • Metabolic Diseases • Neoplastic Diseases • Infection and Infestation -Candida -Herpes simplex -Scabies • Psoriasis
Seborrheic dermatitis • Flaky, white to yellowish scales form on oily areas • Involvement of the top of the scalp (cradle cap), axilla, and diaper area
Allergic Contact Dermatitis • Inflammation of the skin caused by direct contact with an irritating substance • Skin lesion or rash at the site of exposure • Lesions of any type: redness, rash, papules (pimple-like), vesicles, and bullae (blisters) • May involve oozing, draining, or crusting • May become scaly, raw, or thickened • Dx: patch testing • Tx: avoidance, topical steroids Textile dye Uroshiol Nickel Uroshiol
Irritant Contact Dermatitis Irritant contact dermatitis occurs when chemicals or physical agents damage the surface of the skin faster than the skin is able to repair the damage. Irritants include such everyday things as water, detergents, solvents, acids, alkalis, adhesives, metalworking fluids and friction. 47-year-old housekeeper was the result of chronic hand washing combined with surfactant and other solvent exposures
Immunodeficiencies • Wiskott-Aldrich syndrome -X-linked recessive disease -Eczema, thrombocytopenia, and immunodeficiency • DiGeorge syndrome • Hyper-IgE syndrome • Severe combined immune deficiency
Hyper IgE (Job Syndrome) Characterized by recurrent skin abscesses, pneumonia with pneumatocele development, and high serum levels of IgE. Facial, dental, and skeletal features are also associated with this syndrome.