Download
1 / 45
630 likes | 903 Views
Jonathan I. Silverberg, M.D., Ph.D., M.P.H. Assistant Professor, Departments of Dermatology, Preventive Medicine and Medical Social Sciences Director, Northwestern Multidisciplinary Eczema Center Northwestern University, Feinberg School of Medicine Chicago, IL USA. Atopic Dermatitis.

E N D
Jonathan I. Silverberg, M.D., Ph.D., M.P.H. Assistant Professor, Departments of Dermatology, Preventive Medicine and Medical Social Sciences Director, Northwestern Multidisciplinary Eczema Center Northwestern University, Feinberg School of Medicine Chicago, IL USA Atopic Dermatitis.
Disclosures • No relevant financial disclosures or conflicts of interest
Ground rules • At times, I will use the term eczema and atopic dermatitis. These are not actually the same thing. • We will touch upon a number of important topics in eczema, but there is so much more that we wont have time to address.
Structure • What does eczema look like? • How common is eczema? • What are some common risk factors for eczema? • What are some common treatment approaches for eczema? • What health problems occur in patients with eczema?
What does eczema look like? • Ill-defined Hard to delineate where the lesions start and stop • Erythematous Ranges from light pink to flaming red • Patches or Plaques Ranges from flat to very thick plaques
What does eczema look like? • Spongiosis Fluid between cells • Perivascular infiltrate Inflammation around the blood vessels • Eosinophils • asdsad Early or acute eczema
What does eczema look like? • Parakeratosis Scale • Acanthosis Thickening of the epidermis • asdsad Chronic eczema
What does eczema look like? • Eczema is a morphological pattern either visually or microscopically. • There are several types of eczema: • Atopic dermatitis (AD) • Contact dermatitis • Irritant contact dermatitis (ICD) • Allergic contact dermatitis (ACD) • Drug-induced dermatitis • asdsad
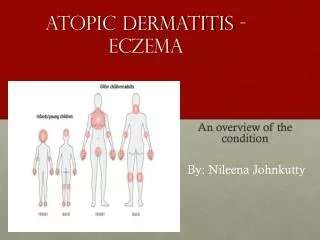
What does eczema look like? Atopic dermatitis Age related changes of distribution: • Infancy: Facial and scalp dermatitis • Toddler: Extensor dermatitis • Older children and adults: Flexural distribution • Adults: More head & neck and hand lesions.
What does eczema look like?Atopic dermatitis Flexural distribution Antecubital and popliteal fossa, anterior neck, wrists, ankles Pathomnomonic Lichenification Accentuation of skin lines Secondary to rubbing and scratching Occurs in chronic lesions Erythema may appear more purple or brown than red in skin of color
What does eczema look like?Atopic dermatitis • Head and neck distribution More common in adults • Hands Often only finding in adults with AD. Katsarou A, Armenaka M. Atopic dermatitis in older patients: particular points. Journal of the European Academy of Dermatology and Venereology : JEADV. 2011;25(1):12-18. • Eyelids Usually accompanied by other signs and symptoms of AD. Case reports of AD presenting exclusively on the eyelids.
How common is eczema? • 1-year prevalence of eczema in US adults is 10.2% Silverberg JI, Hanifin J. Adult eczema prevalence and associations with asthma and other variables: A US population-based study. Journal of Allergy and Clinical Immunology. 2013 Nov;132(5):1132-8. • Remarkably similar to the 10.7% prevalence of eczema found in US children. Shaw TE, Currie GP, Koudelka CW, Simpson EL. Eczema prevalence in the United States: data from the 2003 National Survey of Children's Health. J Invest Dermatol. 2011 Jan;131(1):67-73. • Most common inflammatory skin disease.
Eczema rates vary by state • Silverberg JI. Unpublished data. Statewide prevalence of eczema was divided into tertiles. Data are presented as the percent (95% CI) of subjects who endorsed having eczema in the past 12 months.
Eczema rates vary by age • 2012 National Health Interview Survey Children: 12.0% (11.3-12.7%) Adults: 7.2% (6.9-7.6%) Silverberg JI. Unpublished data.
Distribution of eczema severity (95% CI) • Silverberg JI and Simpson EL. • Pediatric Allergy and Immunology. 2013.
Risk factors for eczema:Race / ethnicity • Higher prevalence in African American children and adolescents. * Rao-Scott Chi square test • Silverberg JI, Hanifin J, Simpson EL. Climatic factors are associated with childhood eczema prevalence in US. Journal of Investigative Dermatology. July 2013. • Similar results observed in: Shaw T, Currie GP, Koudelka CW, Simpson EL: Eczema prevalence in the United States: Data from the 2003 National Survey of Children’s Health. J Invest Dermatol 131:67-73, 2011.
Risk factors for eczema: US birthplace Eczema prevalence Silverberg JI, Simpson EL, Durkin HG, Joks R. Prevalence of allergic disease is lower in foreign-born American children, but increases with prolonged US residence. JAMA Pediatrics. 2013.
Risk factors for eczema: US residence Silverberg JI, Simpson EL, Durkin HG, Joks R. Prevalence of allergic disease is lower in foreign-born American children, but increases with prolonged US residence. JAMA Pediatrics. 2013. • Children born outside the US have significantly lower prevalence of eczema (and other allergic disorders). • Duration of residence in the US is a previously unrecognized factor in the epidemiology of AD.
Risk factors for eczema:Climate Silverberg JI, Hanifin J, Simpson EL. Journal of Investigative Dermatology. 2013.
Risk factors for eczema:Obesity • Recent meta-analysis of 30 studies from across the medical literature. • Obesity was associated with higher rates of eczema in children and adults in North America and Asia. Zhang A and Silverberg JI. Journal of the American Academy of Dermatology. In Press.
Common treatments for eczema • Topical agents • Corticosteroids, e.g. hydrocortisone • Calcineurin inhibitors, e.g. tacrolimus. • Systemic agents • Corticosteroids • Cyclosporine • Mycophenolate mofetil • Tacrolimus • Methotrexate • Azathioprine • Light therapy and lasers • NBUVB, Excimer, PUVA
Systemic corticosteroids • Oral: prednisone, methylprednisolone, etc. • IV: methylprednisolone • Intralesional and intramuscular: Triamcinolone • Rapid onset, dramatic improvement of disease.
Systemic corticosteroids • Horrific adverse effect profile: • Weight gain, Cushingoid habitus, diabetes, hypertension, gastroesophageal reflux, osteoporosis with prolonged use, osteonecrosis even with a single dose, adrenal insufficiency, increased risk of mild and serious infections and malignancy, neurocognitive events including depression and psychosis, fluid overload secondary to mineralcorticoid activity, etc. • More appropriate for contact dermatitis with brief or limited exposures, e.g. poison ivy. • Should be avoided for chronic persistent atopic dermatitis.
Cyclosporine (CsA) • Best evidence for shutting down active disease and preventing flares • Typically works as fast as prednisone, but has longer lasting benefit. • Adverse effect profile not perfect, but better than prednisone: • Hypertension, kidney injury/disease, hyperkalemia, hypomagnesemia, gingival hypertrophy, hypertrichosis, dizziness, GI upset, increased risk of infection, increased risk of solid organ and hematological malignancy especially with prolonged use. • Can only use for limited period of time (6-24 months). • Must monitor blood pressure regularly and check bloodwork periodically.
Methotrexate • Efficacy also established in well-designed trials • Easier dosing: once weekly • Slower onset of action than CsA. Can be used for extended periods. • May not be as effective as CsA at standard doses • Adverse effects: • Anemia/pancytopenia, elevated transaminases and liver fibrosis/failure, GI upset, heavy menstrual bleeding, increased risk of infection and malignancy • Must monitor bloodwork periodically. • Should be given with folic acid 1mg daily
MycophenolateMofetil • Efficacy demonstrated in well-designed trials; however, allowed the most breakthrough flares requiring add-on tx with prednisone • My personal experience: not as effective as CsA or MTX • Generally, better tolerated than other systemics. • Adverse effects: • Anemia, pancytopenia, gastrointestinal discomfort and diarrhea, genitourinary complaints, swelling, increased risk of infection and malignancy, case-report of PMLE.
Azathioprine • Multiple RCT demonstrated efficacy in AD. • Used commonly in Europe. Not as much in US. • Check bloodwork at baseline and periodically. • Can monitor therapeutic levels with blood test. • Adverse effects: • Hypersensitivity with rash, GI upset, increased risk of infections and malignancy, bone marrow suppression.
Cutting edge: Dupilumab • Fully human anti- interleukin 4 receptor alpha antibody • Blocking antibody downregulation of IL4 and IL13 pathways, i.e. Th2 immune responses. • Th2 responses are found in acute and chronic AD skin lesions, asthma, hay fever and food allergies. • Represents first “targeted therapy” for AD • Initial benefit demonstrated in asthma with eosinophilia (NEJM, 2013). • Currently in phase 2B recruitment.
Promise of biologics • The toxicity of the abovementioned systemic agents lies in their blanket immunosuppression. • More targeted therapy may: • Improve efficacy • Eliminate toxicity beyond the immune system • Minimize immunological sequelae with decreased risk of infection and malignancy. • In turn, these open the door for ongoing maintenance therapy for months or even years.
Other biologics being tested • Phase 2 study of a monoclonal anti-IL31 antibody for AD (Chugai). • Phase 1 study of a monoclonal anti-IL31 antibody for AD (Bristol-Myers Squibb). • Both with promising results as treatments for itch in AD and well tolerated.
Other biologics • Intravenous immunoglobulin, omalizumab – evidence does not support efficacy in AD. • AD is a Th2 mediated, but not an IgE mediated disease. • Anti-interleukin 5 antibodies – only modest effects.
Health problems in eczema:Hurts in the wallet • Higher out of pocket (OOP) costs overall. • $32,875,382,250 annual OOP costs in eczema patients. • $502/ year additional OOP cost per patient. Silverberg JI. JAMA Dermatology. In Press.
Health problems in eczema:Hurts in the wallet • 5,898,289 lost workdays for eczema per se • 221,607,545 days in bed for adults with eczema • More doctor visits and ER visits for adults with eczema. • 1 in 4 adults with eczema did not see a doctor for their eczema. Silverberg JI. JAMA Dermatology. In Press.
Health problems in eczema:Sleep disturbance • One third of adults with eczema reported having regular fatigue, daytime sleepiness and insomnia. • Sleep disturbance and fatigue are major players in the poor quality of life, number of sick days and doctor visits in patients with eczema. Silverberg JI,et al. Journal of Investigative Dermatology. 2014.
Health problems in eczema:asthma, hay fever and food allergies Silverberg JI and Simpson EL. Pediatric Allergy and Immunology. 2014.
Health problems in eczema:asthma, hay fever and food allergies Silverberg JI and Simpson EL. Pediatric Allergy and Immunology. 2014.
Health problems in eczema:osteoporosis and fractures. • Children with eczema have lower bone mineral density. Silverberg JI. Pediatric Allergy and Immunology. In Press. • Adults with eczema have: • Lower bone mineral density overall. • Higher rates of osteoporosis. • Higher rates of fractures. Garg NK and Silverberg JI. Journal of Allergy and Clinical Immunology. In Press.
Health problems in eczema:traumatic injuries. • Children with eczema have higher rates of serious injuries requiring medical attention. Garg NK and Silverberg JI. Annals of Allergy, Asthma and Immunology. 2014. Garg NK and Silverberg JI. JAMA Dermatology. 2014.
Health problems in eczema:Irritant contact dermatitis • Not an allergy per se. • Infrequent exposure to strong irritants or frequent exposure to milder irritants. • Often occurs in atopic dermatitis due to impaired barrier and lower irritant threshold. NassifA, Chan SC, Storrs FJ, Hanifin JM. Abnormal skin irritancy in atopic dermatitis and in atopy without dermatitis. Archives of dermatology. 1994;130(11):1402-1407. • Common exposures include: • Frequent hand washing • Hand sanitizers • Harsh soaps, e.g. antibacterial. • Heavily fragrant skin care products.
Health problems in eczema:Allergic Contact dermatitis • Skin allergy. • May become allergic after infrequent exposure to strong allergens or frequent exposure to milder allergens. • Once an allergy develops, even minimal exposures can be provocative. • Delayed reactions that take takes, sometimes weeks, to develop.
Health problems in eczema: Allergic Contact dermatitis & Patch testing • Monday: Patches applied to back with adhesive tape. • Wednesday: Patches removed and placemarker grid is drawn with marker. • Thursday: Final reading. • Sometimes: Monday, Thursday, Monday sequence
Northwestern Multidisciplinary Eczema Clinic • Rationale • 15.7% of adults with eczema have active hay fever • 21.1% of adults with eczema have a history of asthma, of which 40.8% had an asthma attack in past year. Silverberg JI, Hanifin J. Adult eczema prevalence and associations with asthma and other variables: A US population-based study. Journal of Allergy and Clinical Immunology. 2013 Nov;132(5):1132-8. • One third of adults with eczema have sleep disturbances that cause poor quality of life. Silverberg JI, Garg NK, Paller AS, Fishbein A, Zee PC. Sleep disturbances in adults with eczema are associated with impaired overall health: A US population-based study. Journal of Investigative Dermatology. 31 July 2014; doi: 10.1038/jid.2014.325. • Eczema is associated with significant psychological comorbidities and behavioral problems, including depression, anxiety and attention deficit (hyperactivity) disorder. Gark NK, Silverberg JI. Association between childhood allergic disease, psychological comorbidity and injury requiring medical attention. Annals of Allergy, Asthma and Immunology. 2014 Jun. 112(6): 525-32.
Northwestern Multidisciplinary Eczema Clinic • Monthly clinic • Providers from Dermatology (Silverberg), Allergy-Immunology (Peters and Grammer) and Neurology-Sleep Medicine (Attarian). • Psychiatry will be joining soon (Franks). • Services provided include: • Consultation and treatment. • Patch testing for allergic contact dermatitis. • Skin prick testing for seasonal and food allergies. • Spirometry for asthma assessment. • Actigraphy for assessment of sleep disturbances.
Northwestern Multidisciplinary Eczema Clinic • History • First session in May, 2014 • Seen >70 patients from 6 states to-date. • Provided unique insight into the comorbidities of atopic dermatitis, resulting in two research grant submissions.
Thank you. Questions??