Download
1 / 29
290 likes | 692 Views
Vein of Galen. Clinical Case Presentation Marissa Hampton SNNP, RN, BSN University of Texas Medical Branch at Galveston School of Nursing NNP Concepts and Practicum II GNRS 5632 Dr. Debra Armentrout PhD, RN, MSN, NNP-BC Dr. Leigh Ann Cates PhD, APRN, NNP-BC,RRT-NPS,CHSE. Objective.

E N D
Vein of Galen Clinical Case Presentation Marissa Hampton SNNP, RN, BSN University of Texas Medical Branch at Galveston School of Nursing NNP Concepts and Practicum II GNRS 5632 Dr. Debra Armentrout PhD, RN, MSN, NNP-BC Dr. Leigh Ann Cates PhD, APRN, NNP-BC,RRT-NPS,CHSE
Objective • Identify the high risk neonate • Integrate pertinent patient information in developing a plan of care. • Review the infants systems by hospital course. • Discuss current theory and research as related to the infants primary medical diagnosis
Maternal History • Caucasian, 25 year old mother • Gravida 2, Para 1 • History of previous miscarriage at 8 weeks with same father of infant • Estimated date of delivery: 5/1/2014 • Adequate prenatal care • Known vein of Galen malformation seen on prenatal ultrasound • Including follow up with pediatric cardiologist • O + blood type • Negative maternal labs • Human Immunodeficiency Virus (HIV) • Unknown maternal labs (awaiting arrival from office) • Group Beta Strep (GBS) • Rapid plasma reagin (RPR) serology • Rubella • Hepatitis B status (HBsAg) • Denies tobacco, alcohol and illicit drug use • Married
Maternal and Fetal Risks and Complications • Vein of Galen malformation • Potential fetal complications • Most complications arise after delivery due to altered blood flow and vascular resistance • Congestive Heart Failure • Pulmonary Hypertension • Myocardial ischemia • Cerebral edema • Renal failure • Obstructive hydrocephalus • Related to size, position of malformation and compression on brain structures (Hoang, Choudhri, Edwards & Guzman, 2009) (Gomella, Cunningham & Eyal, 2013) (Geneva Foundation for Medical Education and Research, 2014)
Maternal and Fetal Risks and Complications • Unknown maternal labs • Maternal risk • Low suspicion due to adequate prenatal care • Possible untreated sexually transmitted disease, group b strep infection or liver damage • Fetal risk • At risk for Hepatitis B transmission • At risk for GBS septicemia • At risk for congenital syphilis • At risk for congenital abnormalities due to rubella infection
Delivery and stabilization • Elective Cesarean Section • Due to Congenital Anomalies • Epidural Anesthesia • Rupture of Membranes at delivery with clear fluid • Vertex Presentation • Apgars • 8 at one minute of life • 9 at 5 minutes of life • Delivery summary: • Infant pink, crying, vigorous at delivery • Drying and tactile stimulation provided • Adequate respiratory effort, with initial HR >100 • Infant remained stable with good tone, reflex, color and adequate respiratory effort through out stabilization and during transfer to NICU
Admission Assessment and Diagnostics • Birth Gestation 38.4 weeks • Gender: Male • Birth weight: 3450 grams (51-75%tile) • Head circumference: 35.5 cm (76-90%tile) • Length: 52 cm (76-90%tile) • Admission vital signs • Temperature 99.3 F • Heart rate 172 bpm • Respiratory rate 44, O2 saturation 91% on 4 liters per minute (LMP) • Blood pressure: 57/34 (40) • Admission Physical Exam: • General: Active and alert, responsive to exam. • Head/EENT: Bilateral red reflexes noted. Normocephalic. AFSF. No cleft deformities. Bruit present in anterior fontanels • Lungs: Clear bilateral breath sounds with mild subcostal retractions. • Heart: Regular rate and rhythm, without murmur, pulses 3+. Decreased perfusion. • Abdomen: Soft, round, active bowel sounds. No organomegaly. 3 vessel cord. • Genitalia: Normal external male genitalia with bilateral descended testicles. Patent anus. Spine intact. • Extremities: Full range of motion in extremities. Hips without click bilaterally. • Skin: Pink and warm without pathologic lesions.
Admission Assessment and Diagnostics • Diagnostics: • Chest x ray • Clear bilateral lung fields with adequate lung volumes, expansion to T 9 • Enlarged cardiac silhouette • Head ultrasound • Vein of Galen malformation 12 mm in diameter • Admission Blood Culture • Results pending for 48 hours- Negative • Complete blood count (CBC) • White blood cell count: 9.8 • Hemoglobin/ Hematocrit: 12.3% / 36.9% • No left shift • Blood glucose • Initial: 37 mg/dl • Repeat following bolus: 47 mg/dl • Follow up blood sugar after second D10 W bolus and initiation of IVF: 75mg/dl • Arterial Blood gas • Initial pH 7.28 pCO2 59.2 pO2 49 HCO3 27.6 BE 1 • Mild respiratory acidosis
Primary Admission Diagnosis • 38 week AGA male infant • Arteriovenous Malformation- Vein of Galan • Transient Hypoglycemia • Respiratory Distress • Suspected sepsis (Geneva Foundation for Medical Education and Research, 2014)
Etiology: ~ 1 in 25,000 • Vein of Galen • Arteriovenous (AV) malformation with shunting of blood • Improperly named • Persistent embryonic vein • Congenital aneurysmal malformation of the vein of Markowski • Aneurysm forms in stages with development of cerebral vascular system • Stage I: Neural cells/tube receive nutrients from amniotic fluid • Stage II: Neural matter/ vascular channels develop • Stage III: Developing brain matures, cerebral veins develop and drain into the vein of Markowski. Vein of Markowski should involute; persistence of great vein is now termed Vien of Galen. Etiology and Pathophysiology of primary admission diagnosis • Etiology: ~ 1 in 25,000 • Vein of Galen • Arteriovenous (AV) malformation with shunting of blood • Improperly named • Persistent embryonic vein • Congenital aneurysmal malformation of the vein of Markowski • Aneurysm forms in stages with development of cerebral vascular system • Stage I: Neural cells/tube receive nutrients from amniotic fluid • Stage II: Neural matter/ vascular channels develop • Stage III: Developing brain matures, cerebral veins develop and drain into the vein of Markowski. Vein of Markowski should involute; persistence of great vein is now termed Vien of Galen. (Hoang, Choudhri, Edwards & Guzman, 2009) (Li, Armstrong, terBrugge, 2011) (Sheth, 2014)
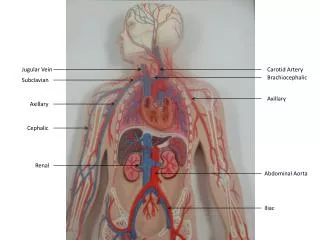
Etiology and Pathophysiology of primary admission diagnosis • Vein of Galen is located under the cerebral hemispheres • Drains the anterior and central regions of the brain into the sinuses of the posterior cerebral fossa. • Lesion is midline and receives bilateral blood supply from collateral circulation • Two types of AV malformation • Choriodal malformation • Leads to severe vessel malformation and symptoms • Extensive arterial network • Mural malformation • Multiple high flow shunts that end within the vein of Markowski • Occurs 6th- 11th week of gestation (Khullar, Andeejani, & Bulsara, 2010)
Etiology and Pathophysiology of primary admission diagnosis • Pathophysiology • In utero • Low resistance rarely • After birth • Changes in blood flow due to changing resistance • Cerebral venous congestion causes: • Abnormal cerebral spinal fluid (CSF) flow • High blood flow shunts to the vein of Galen and reduces flow to the cerebral parenchyma • Decreased blood flow to the brain results in cerebral edema • May cause rapid loss of brain tissue • Leads to impaired resorption of CFS resulting in hydrocephalus • Cardiac failure due to increased venous return • Low resistance venous shunt to vein of Galen increases venous return to right atrium • Increased pulmonary blood flow causes pulmonary hypertension • Congestive heart failure (Hoang, Choudhri, Edwards & Guzman, 2009)
Initial Plan of Care • Admit infant to NICU via radiant warmer. • Cardiopulmonary monitoring, pulse oximetry monitoring. • Admission weight, length, frontal occipital circumference (FOC). • Admission vital signs every (q) 15 minutes x4, q 30 minutes x 4, q hourly x 4, then q 3 hours. • Admission 4 point blood pressures (bp). • Strict intake and output. • Infuse D12.5W + 1 meq Ca gluconate/100ml + 0.25 units of heparin/ ml via umbilical venous catheter(UVC) to run at 10 ml/hour. • Infuse ½ Normal Saline(NS) + 0.25 units of heparin via umbilical arterial catherter (UAC) at 1 ml/hr. Total IVF ~ 80 ml/kg/hr. • Monitor bp via UAC. Notify if mean bp is <35 or >65. • Administer 6.9 ml of D10 IV bolus x 1, repeat bedside blood sugar level in 30 minutes. • Initiate feeds of expressed breast milk or Similac Advance 20 kcal/oz 15ml q 3 hours by mouth (PO) or orogastric tube (OGT)
Initial Plan of care • 4 liters per minute (LPM) high flow nasal cannula (HFNC) • Titrate Fio2 to remain in target saturations (92-96%). • Stat Chest /abdominal x-ray. • Routine echocardiogram. • Stat head ultrasound. • AM magnetic resonance imaging (MRI) and MRA • Obtain maternal labs. • Begin Lasix 1mg/kg PO q 24 hours • Obtain and follow admission lab work: • Blood culture, Complete blood count (CBC), C-reactive protein (CRP) • Q 6 hour bedside glucoses once blood sugars are stable • In AM obtain: • Basic metabolic panel (BMP), Total/direct bilirubin level, CBC, CRP
Hospital course by system Neurology • Known vein of Galen malformation • Detected in utero via ultrasound • Head ultrasound(HUS) performed on admission • 12 mm in diameter • Mild cardiomegaly in conjunction with malformation via echo • Pulsating anterior fontanel with bruit • MRI/MRA performed on admission • MRI revealed vein of Galen malformation with posterior feeding vessels • No hydrocephalus • Pediatric Neurosurgery/ Neuroradiology consulted • Planned ablation in 2-6 months due to stable aneurysm • Follow up HUS at 3 weeks of age • No hydrocephalus
Hospital course by system Pulmonology • Initial respiratory distress after delivery • Possibly due to retained lung fluid from elective c section • Required up to 4LPM due to desaturations (Fio2 titrated) • Development of pulmonary edema secondary to cardiac failure from vein of Galen malformation • Low dose Lasix continued • Improvement of capillary blood gases with decreased Fio2 needs • Infant tolerated daily flow wean on nasal cannula (NC) • Inhaled nitric oxide initiated for probable persistent pulmonary hypertension (PPHN) • Confirmed by echocardiogram • iNO initiated after a dysrhythmia event, increased flow and Fio2 requirements elevated brain natriuretic peptide (BNP) and worsening echocardiogram results • Trial recommended by cardiology, short term use • Gradual wean of iNO and NC • Follow up echocardiograms obtained • Room air status • Post operative O2 needs after G button replacement • Evidence of pulmonary edema and cardiomegaly • Continued Lasix administration, NC, fluid restriction • Room Air status • Sildenafil initiated
Hospital course by system Cardiology • Known arteriovenous malformation • Vein of Galen diagnosed in utero via ultrasound • Enlarged heart seen on x ray • Lasix administration initiated • BNP monitored • Admission Echocardiogram • Revealed moderate patent ductus arteriosus (PDA), mild PPHN and dilated right ventricle • Repeat Echocardiogram the next day • Closing PDA with right to left shunting • Suprasystemic PPHN • Initiated trial of iNO at 20 ppm • Dilated right ventricle • Episode of Supraventricular tachycardia noted • Resolved with vagal maneuver • Cardiology consulted • Follow up echocardiogram • Improving contractility and decreased pulmonary pressures • BNP continues to improve • Final echocardiogram • PDA is closed • Some persistent PPHN with bidirectional shunting via the PFO/ASD • Home regimen of sildenafil
Hospital course by systems Gastrointestinal system: • Initial hypoglycemia resolved with two D10 boluses • D10 W IVF administration via UVC • Small bolus feeds initiated on DOL 1 • Initially at 40 mg/kg/day then advanced daily to 160 mg/kg/day • Hypoglycemia resolved • Hyponatremia acquired secondary to lasix administration • Supplemental NaCl initiated in feeds • PO ad lib feeds prior to discharge • Poor feeder • Infant failed 2 day rooming in process by only completing 125 m/kg/day • Insufficient volume and caloric intake • Family decides on G button placement • Consulted with pediatric surgery • G button placement for home management • PO adlib feeds with remainder of volume given via g button
Hospital course by system • Genitourinary • Unremarkable • Musculoskeletal • Unremarkable • Hematological • Unremarkable • Adequate hct levels • No transfusions during hospital stay • Ophthamology • Unremarkable • Infectious disease • Initial blood culture negative at 48 hour • Once obtained all of mothers prenatal labs were negative • Low risk for suspected infection
Medications On admission: • Vitamin K intramuscular (IM) injection, 1 mg x 1 • Erythromycin ophthalmic eye ointment OU x 1 • Lasix • Began on admission for congestive heart failure • 1 mg/kg PO q 24 hours, then increased to 1 mg/kg PO q 12 hours History of: • Normal saline bolus IV at 10mg/kg at admission • D10W IVF for initial hydration at admission • Sodium chloride for hyponatriemia • 2 mEq PO q 8 hours, then increased to 4 mEq PO q 8 hours • Ancef prior to g button placement • 100 mg IV q 8 hours • Morphine for pain control post op • 0.1 mg/kg IV Q 4 hrs PRN • Versed for agitation prior to MRI • 0.25 mg IV
Medications • Hepatitis B vaccine 5mcg IM x 1 Current medications • Sildenafil 0.5 mg/kg q 6 hours PO • Tylenol 40 mg/kg PRN for pain related to circumcision
Pertinent theories and Evidence based practice • Vein of Galen • Composes about 1% of all intracranial vascular lesions • About 30% of these lesions are discovered in neonates • Historically, grave prognosis • First case described in 1949 • As of 1982, infant with vein of Galen had a 100% intraoperative mortality rate • Development of endovascular techniques began in early 1980s • By 1991 mortality rate for endovascular procedures decreased to 50% • By 1993 mortality rate decreases dramatically • Due to advances in embolization technique • Although mortality rates decreased dramatically, normal cognitive development was not always preserved • Currently neurological function with therapy may be abnormal in 50 % of survivors. (Zahka & Gruenstein, 2013) (Khullar, Andeejani& Bulsara, 2010) (Heuer, Gabel, Beslow, Stiefel, Schwartz, Storm., … & Hurst, 2009)
Pertinent theories and Evidence based practice • Multiple studies emphasize that untreated infants have a poor prognosis • Mortality rate of 75 % • Prognosis is related on age • Infants who require endovascular treatment within the first month of life have the worse prognosis • Highest rates of mortality and neuro/developmental delays • Highest success rates if embolism is prolonged to 5-6 months of age • Increased efficacy of embolization procedure • Small risk to brain maturation • Reports of spontaneous resolution are rare (Khullar, Andeejani, & Bulsara, 2010) (Geneva Foundation for Medical Education and Research, 2014
Pertinent theories and Evidence based practice • Improvements in endovascular therapy, antenatal diagnosis and neonatal critical care have improved outcomes • First consider medical management • Treat congestive heart failure • Inotropes for renal stability • Diuretics to decrease cardiac load • Fluid restriction • Endovascular treatment • Goal is to obliterate lesion by endovascular occlusion • ~ 60% of neonates with endovascular treatment have had minimal to no developmental delay at follow up • Complete occlusion is not necessary • Partial embolization may cause thrombosis • Surgical treatment is only used with embolization failure • Primary treatment was open microsurgery • Low success rate (Blount, Oakes, Tubbs & Humphreys, 2006) (Moftakhar, Damielpour, Maya & Alexander, 2009)
Family interaction • Mother and father of baby remained closely involved in infants care. Family visited daily and participated in infants cares such as feeding, bathing and bonding. Parents participated in a two day room in prior to the first anticipated discharge date. Infant failed to complete feeds and only took about 120 ml/kg/day. Parents discussed at length infants feeding options with his primary neonatalogist and opted for a planned G button. Surgery for button placement was made for the end of the week. Infant’s rooming in was cancelled, and plan of care continued until surgery. Post operative care and problems were discussed with the family at length. Parents remain cooperative through out the infants stay and plan of care.
Discharge plan and follow up • Discharge Plan • Infant is not currently ready for discharge, but upon discharge will: • Continue PO adlib feeds, g button feed when infant does not finish volume • Circumcision care after surgery (g button placement) • Hearing screen passed • Discharge infant home in care of parents • Follow up appointments • Pediatrician appointment • Follow up as outpatient with surgery at one month for gbutton placement • Follow up with interventional neuroradiology at 2 months of life to consider ablation • Follow up with pediatric neurosurgery at 2 months of life to consider ablation
Summary • Early intervention is necessary to avoid a poor prognosis. • Medical management should always be considered first. • Avoidance of embolization until the 5th-6th month of life has most desirable outcomes. • Avoiding surgery can only be accomplished if infant remains hemodynamically stable. • Interdisciplinary team should be established to guide infants care. • Includes Neonatologist, Neuroradiology, Neurosurgery, and nursing.
References • Blount, J. P., Oakes, W. J., Tubbs, R. S., Humphreys, R. P. (2006). History of surgery for cerebrovascular disease in children. Part II. Vein of Galen malformation. Neurosurgery Focus (6), 1-6. • Geneva Foundation for Medical Education and Research (2014). Vein of Galen malformation. Retrieved from http://www.gfmer.ch/genetic_diseases_v2/gendis_detail_list.php?cat3=42 • Gomella, T. L, Cunningham, M. D. & Eyal, F. G. (2013). Neonatology: Management, procedures, on-call problems, diseases and drugs (7th Ed.). New York: McGraw Hill Education • Heuer, G. G., Gabel, B., Beslow, L. A., Stiefel, M. F., Schwartz, E. S., Storm, B. P., Ichord, R. N., & Hurst, R. W. (2009). Diagnosis and treatment of vien of Galen malformations. Childs Nervous System. doi: 10.1007/s00381-009-1063-8 • Hoang, S., Choudhri, O., Edwards, M., & Guzman, R. (2009). Vein of Galen malformation. Neurosurgery Focus, 27 (5), 1-6. doi: 10.3171/2009.8FOCUS09168 • Khullar, D., Andeejani, A., Bulsara, K. R. (2010). Evolution of treatment options for vein of Galen malformations. Journal of Neurosurgery: Pediatrics 6, 444-451. doi: 10.317/2010.8.PEDS10231 • Li, A., Armstrong, D., terBrugge, K. G. (2011). Endovascular treatment of vein of Galen aneurysmal malformation: management strategy and 21 year experience in Toronto. Journal of Neurosurgery: Pediatrics (7), 3- 10. doi: 10.3171/2010.9.PEDS0956
References • Moftakhar, P., Danielpour, M., Maya, M., & Alexander, M. J. (2009). Spontaneous thrombosis of neonatal vein of Galen malformation. Neurosurgery Focus, 27(5), 1-5. doi:10/3171/2009/.8.FOCUS09162) • Sheth, R. D. (2014). Vein of Galen malformation. Medscape Retrieved from http://emedicine.medscape.com/article/1179888-overview#showall • Zahka, K. G., & Gruenstein, D. H. (2011). Approach to the neonate with cardiovascular disease. In R. J. Martin, A. A. Fanaroff, & M. C. Walsh (Eds.), Neonatal-Perinatal Medicine: Diseases of the fetus and infant (9th ed., pp. 1215-1222). Philadelphia, PA: Mosby Elsevier