Download

1 / 45
450 likes | 562 Views
IMMUNE SYSTEM. PECULIARITIES of ITS FUNCTIONING. INSPECTION METHODS IN CHILDREN. SEMIOTICS. С ARE FOR PATIENTS.

E N D
IMMUNE SYSTEM. PECULIARITIES of ITS FUNCTIONING. INSPECTION METHODS IN CHILDREN. SEMIOTICS. СARE FOR PATIENTS
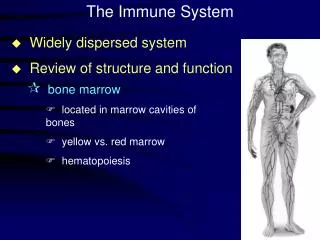
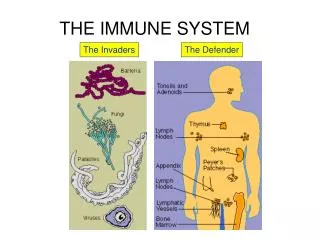
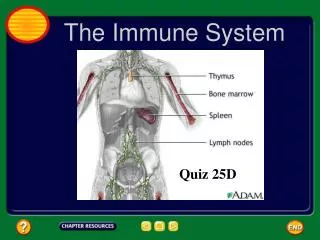
The immune system includes the primary lymphoid organs (thymus, bone marrow, and probably liver) and the secondary lymphoid organs (lymph nodes, spleen, and gut-associated lymphoid tissue [GALT]).
The functions of the immune system are basically two types: nonspecific and specific. Nonspecific immune defenses are activated on exposure to any foreign substance but react similarly regardless of the type of antigen; they are unable to identify the antigen. The principal component of this system is phagocytosis, the process of ingesting and digesting foreign substances. Phagocyte cells are composed of neutrophils and monocytes
Specific defenses are those that have the ability to recognize the antigen and respond selectively. The components of adaptive immunity are humeral immunity and cell-mediated immunity. The cells responsible for these two forms of immunity are the lymphocytes, specifically B-lymphocytes and T-lymphocytes.
Humoral immunity Humeral immunity is involved with antibody production and complement. The principal cell involved in antibody production is the B-lymphocyte.Five classes of antibodies or immunoglobulins (lg) have been identified: G, M, A, D, and E, each serving a specific function . On initial exposure to an antigen, the B-lymphocyte system begins to produce antibody, predominantly lgM, which appears in 2 to 3 days. This process is referred to as the primary antibody response.
Cell-mediated immunity Cell-mediated immunity is involved in a variety of specific functions mediated by the T-lymphocyte. The T-lymphocyte is so named because it passes through the thymus during the differentiation process, which leads to the mature T-cell. T-lymphocytes do not carry typical immunoglobulins on their surfaces as do the B-cells. However, they are functionally heterogeneous in that several subsets have been identified, including cytotoxic T-cells, memory T-cells, helper T-lymphocytes, and regulator T-lymphocytes.
Cell-mediated immunity Specific functions of T-lymphocytes include: • protection against most viral, fungal, and protozoan infections and slow-growing bacterial infections, such as tuberculosis, • rejection of histoincompatible grafts, mediation of cutaneous delayed hypersensitivity reactions, such as in tuberculin testing, • and probably immune surveillance for malignant cells. • In addition, they also have regulatory functions within the immune system.
Cell-mediated immunity The immunologic system undergoes numerous changes during the first year. The newborn receives significant amounts of maternal lgG, which confers immunity for about 3 months against antigens to which the mother was exposed. During this time the infant begins to synthesize his own lgG, and about 40% of adult levels are reached by 1 year of age. Significant amounts of lgM are produced at birth, and adult levels are reached by 9 months of age. The production of IgA, IgD, and IgE is much more gradual, and maximum levels are not attained until early childhood.
Cell-mediated immunity Immunoglobulin G (lgG), which neutralizes microbial toxins, reaches adult levels by the end of the second year of life. Passive immunity from maternal transfer disappears by the beginning of toddlerhood, necessitating the use of artificial immunizations. Immunoglobulin M (lgM), which responds to artificial immunizing techniques and combats serious infection, attains adult levels during late infancy. Immunoglobulins A, D, and E increase gradually, not reaching eventual adult levels until later childhood. Many young children demonstrate a sudden increase in colds and minor infections when entering nursery school or kindergarten because of the exposure to new antigens.
The terms in immunology • immunity An inherited or acquired status in which an individual is resistant to the occurrence or the effects of a specific disease, particularly an infectious agent. • natural immunity Innate immunity or resistance to infection or toxicity. • acquired immunity Immunity from exposure to the invading agent, either bacteria, virus, or toxins.
The terms in immunology • active immunity: individual actively forms immune bodies against specific antigens, either naturally by his having had the disease clinically or subclinically or articifically by the introduction of an antigen (vaccine) into the individual. • passive immunity: temporary immunity by transfusing plasma proteins either artificially from another human or an animal that has been actively immunized against an antigen or naturally from the mother to the fetus via the placenta. • antibody: a protein found mostly in serum that is formed in response to exposure to a specific antigen.
The terms in immunology • antigen: a variety of foreign substances, including bacteria, viruses, toxins, and foreign proteins that stimulate the formation of antibodies. • antitoxin: antibody formed in response to a toxin (antigen). • toxin: a poisonous substance usually produced by the invading microorganism. • toxoid: a toxin that has been treated to destroy its toxic properties but retain its antigenic quality.
The terms in immunology • vaccine: collectively a term to denote any type of active immunization, such as toxoids or attenuated live viruses; specifically a suspension of disease-causing bacteria or viruses that acts like an antigen, stimulates antibody production, and produces active acquired immunity. • attenuate: reduction of the virulence (infectiousness) of a pathogenic microorganism by such measures as treating it with heat, chemicals, or cultivating it on a certain media.
Specific (adaptive) defenses are those that have the ability to recognize the antigen and respond selectively. The components of adaptive immunity are humoral immunity and cell-mediated immunity. The cells responsible for these two forms of immunity are the lymphocytes, specifically B-lymphocytes and T-lymphocytes
Normal development of the immune system After birth, the infant is rapidly colonised by organisms and challenged by waves of transient pathogens. Cellular immunity is active from birth, and although the neutrophil count is relatively low, infants are able to respond to bacterial infection with a leucocytosis. Humoral immunity is less well developed but the maturing system is initially supported by transplacental maternal-derived IgG antibodies and potentially by breast milk factors including IgA. Ig M does not cross the placenta but infants can produce it in response to infection. In an intact immune system the waning ofmaternally derived IgG is matched by gradual enhancement of endogenous production but there is a nadir of circulating IgG levels at age 2-3 months. The emergence of specific endogenous antibodies reflects the process, of natural immunisation, and this is accelerated during the preschool years as children average 6-12 short-lived infections each year.
Abnormal development of the immune system Immunodeficiency is suggested bya history of unusually frequent or severe infections, or by unusual patterns of infection especially if caused by organisms of low pathogenicity. A positive family history is also a powerful guide. Failure to thrive rather than overt infection may be the main manifestation. Modern immunology laboratories are equipped with the tools to test the integrity of each of the main pathways of the immune system, and the classification of disorders has become increasingly functional. Successful management depends upon swift recognition and classification of the disorder, initiation of specific treatments where indicated and meticulous attention to bacteriological and virological investigation of all infectious episodes. Where indicated, life-long immunoglobulin replacement can be very effective.
Clinical manifestations Obviously the most common manifestation is susceptibility to infection early in life, most often by 3 months of age when maternal immunity is low. Specifically the disorder in children is characterized by chronic infection, failure to completely recover from an infection, frequent reinfection, and infection with unusual agents. In addition, the history reveals no logical source of infection. Failure to thrive is a consequence of the persistent illnesses.
If the child should receive a foreign tissue, such as blood supplements, signs of graft-versus-host assey reaction, such as fever, skin rash, alopecia, hepatosplenomegaly, and diarrhea, are expected. Since the reaction requires 7 to 20 days for tissue damage to become evident, the symptoms may be mistaken for an infection. However, the presence of a graft-vs-host reaction increases the child's susceptibility to overwhelming infection and, therefore, is a grave complication.
Diagnostic evaluation Diagnosis is usually based on a history of recurrent, severe infections from early infancy, a familial history of the disorder, and specific laboratory findings, which include lymphopenia, lack of lymphocyte response to antigens, and absence of plasma cells in the bone marrow. Documentation of immunoglobulin deficiency is difficult during infancy because of the normally delayed response of the infant to produce his own immunoglobulins and maternal transfer of immunoglobulin G.
Initial Immunologic Testing of the Child with Recurrent Infections Complete Blood Count, Manual Differential, and Erythrocyte Sedimentation Rate • Absolute lymphocyte count (normal result makes T-cell defect unlikely) • Absolute neutrophil count (normal result precludes congenital or acquired neutropenia and (usually) both forms of leukocyte adhesion deficiency, in which elevated counts are present even between infections) • Platelet count (normal result excludes Wiskott-Aldrich syndrome) • Howell-Jolly bodies (presence suggests asplenia) • Erythrocyte sedimentation rate (normal result indicates chronic bacterial or fungal infection unlikely) Screening Tests for B-Cell Defects • IgA measurement; if abnormal, IgG and IgM measurement • Isohemagglutinins • Antibody titers to tetanus, diphtheria, H. influenzae, and S. pneumoniae
Initial Immunologic Testing of the Child with Recurrent Infections Screening Tests for T-Cell Defects • Absolute lymphocyte count (normal result indicates T-cell defect unlikely) • Candida albicans intradermal skin test: 0.1mL of a 1:1,000 dilution for patients older than 6 yr, 0.1mL of a 1:100 dilution for patients younger than 6 yr Screening Tests for Phagocytic Cell Defects • Absolute neutrophil count • Respiratory burst assay Screening Test for Complement Deficiency • CH50
Diagnostic criteria of primary immunodeficient conditions Clinical: A. Suggestive T-cell deficit: a) systemic illness following vaccination with any alive virus or BCG; b) unusual life-threatening complication following infection caused by ordinary benign viruses (e.g., giant rubella pneumonia; varicella pneumonia); c) chronic oral candidiasis after 6 months of life; d) chronic mucocutaneous candidiasis; e) fine, thin hair, short-limbed dwarfism with characteristicradiographic features of cartilage-hair hypoplasia (CHH); f) intrauterine graft-versus-host disease - the most characteristicfeature is scaly erythroderma and total alopecia (absence of eyebrowsis quite striking); g) graft-versus-host disease after blood transfusion; h) hypocalcemia in newborn (Di George anomaly, especially with characteristic faces, ears and cardiac lesions); i) small (less than 10 mm in diameter) lymphocytes count persistently less than 1500/mm3, must rule out gastrointestinal loss of them or loss from the lymphatic vessels.
Diagnostic criteria of primary immunodeficient conditions B. Suggestive R-cell defect a) recurrent proved bacterial pneumonia, sepsis or meningitis; b) nodular lymphoid hyperplasia. C.Suggestive B- and T-cell deficiency (combined immunodeficientdisease - CID) a) all the above mentioned features except chronic mucocutaneous candidiasis and nodular lymphoid hyperplasia; b)features of Wiskott-Aldrich syndrome (draining ears, trombocyto-penia and eczema); c) features of ataxia-telangiectasia. P. Suggestive immunodeficiency without clearly implicating T-or B-cell defect a) Pneumocystis carinii pneumonia; b) intractable eczema; c) ulcerative colitis in infants less than 1 year old; d) intractable diarrhea; e) unexplained hematological deficiency (RBC, WBC, platelet); f) severe generalized seborrheal dermatitis (Leiner's disease) suggestsC5 deficiency; seborrhea is common in combined immunodeficient disease; g) recurrent pyogenic infections seen in C3 deficiency.
Diagnostic criteria of primary immunodeficient conditions E.Suggestive biochemical defect a) features of combined immunodeficiency with characteristic bony lesions (adenosine deaminase deficiency); b) features of Blackfan-Diamond aplastic anemia (nucleoside phosphorylase deficiency). F.Suggestive abnormality of polymorphonuclear leukocytes a) primary skin infections (if associated with asthma, eczema and coarse faces, think of Buckley syndrome); b) chronic osteomyelitis caused by Klebsiella or Serratia species, draining lymph nodes (chronic granulomatous disease). G.Suggestive secondary deficiency a) concomitant or preceding viral infection; b) lymphoid malignancy (chronic lymphatic leukemia, Hodgkin's disease, myeloma).
Diagnostic criteria of primary immunodeficient conditions Laboratory: a) genealogical anamnesis; b) common blood analysis (not only total but absolute quantityof different leukocytes); c) investigation of numeral link of immunity: • gamma globulin concentration; • immune serum globulins by Manchini; • Immunoelectrophoresis of serum proteins; • tillers of different antibodies, blood group, liter of isohemagglu-tinins; • secretory immunoglobulins; • surface immunoglobulins of antiserum lymphocytes, marked with fluoroscein; • EAC-rosellas. d) investigation of cellular link of immunity: • E-rosellas; • reaction of blast transformation (in unspecific stimulation with FHA, in stimulation with antigens, in mixed lymphocyts culture); • depression of macrophages migration; • reaction of hypersensitivity of a delayed type (intracutaneous tests with 2,4-dinitroftorbenzol, streptokinase, odoriase, antigen; Shieck's reaction).
Diagnostic criteria of primary immunodeficient conditions e) special investigations: • functions of T-helpers and T-suppressors; • hystochemical determination of adenosine-deaminase's activity; • transcobalamin's content. • X-ray of the chest including side positions and tomo-gram of mediastinum for revealing the thymus; • biopsy of the lymph nodes with the use of hystotogical and hystochemical methods; h) investigation of complement's system (total complement, its factors); i) investigation of phagocytosis function (opsonization bacteria's killing, a test with blue tetrazolium, cytochemical methods of determination of enzyme's activity etc.)
Primary immunodeficient conditions. Classification of primary immunodeficient conditions 1. Prevalence of antibodies deficiency: a) sex-linked agammaglobulinemia; b) sex-linked agammaglobulinemia and growth hormone deficiency; c) autosomal recessive agammaglobulinemia; d) selective immunoglobulin deficiency: - with elevated level of IgM and IgD; - IgA deficiency. e) selective deficiency of other isotypes of Ig; f) kappa-chains deficiency; • immunodeficiency on the background of thymoma; • transitory hypogammaglobulinemia in children.
Primary immunodeficient conditions. Classification of primary immunodeficient conditions 2. Combined immunodeficiency: a) total variable immune deficiency: with primary antibody deficiency; with primary deficiency of cellular immunity. b) severe combined immunologic deficiency: - reticular dysgenesis; -deficiency of T- and B-lymphocytes (earlier the Swiss type of IDC). c) T-lymphocyte deficiency (earlier Nezelof syndrome); d) adenosindeaminase deficiency; e) purine-nucleotide-phosphorylase deficiency; f) absence of HLA-antigens of the 1st class (syndrome of "naked"lymphocytes); g) absence of HLA-antigens of the 2nd class.
Primary immunodeficient conditions. Classification of primary immunodeficient conditions 3. Immunodeficiency in combination with other congenital defects: a) Wiscott-Aldrich syndrome; b) ataxia-telangiectasia (Louis-Bar, syndrome); c) syndrome of 3nd-4,h pockets of branchial arch (Di George syndrome); d) transcobalamin-2 deficiency; e) mmunodeficiency due to congenital anomalous reaction at Epstein-Barr virus.
Therapeutic management The only definitive treatment is a histocompatible bone marrow transplant. The perfect donor is an identical twin because the human lymphocyte antigens (HLA) are exactly the same. The second best choice is a sibling. The procedure consists of aspirating several samples of bone marrow from the donor and infusing the marrow intravenously into the host. However, bone marrow transplants are usually done at medical centers where measures to control posttransplantation infection, such as a sterile environment, and other specialized facilities are available. Since the host's immunologic system is incompetent, graft rejection is not a problem. However, a graft-vs-host reaction is always a possibility in a nonidentical twin graft, and once it occurs, little can be done to reverse the process.
IMMUNISATION Protection against some of the infectious diseases is available in the form of immunization which is given at various stages during childhood. Immunizations for different diseases are scheduled tobalance the risks of disease with the child's ability to produce a good immunological response; Immunization should not be given if the child is acutely unwell or if a severe reaction has occurred to a previous dose of that vaccine. Live attenuated vaccines (e.g. poliomyelitis, measles, mumps, rubella, BCG) should not be given to children" with immune deficiency states including those on cytotoxic drugs and high doses of corticosteroids, because of the risk of severe generalised infection. Three weeks should elapse between live vaccines to ensure adequate immune responses to the second one.
National immunisation scheduleDerived from Salisbury DM, Begg NT 1996 Immunisation against infectious disease- Department of Health, HMSO, London INFANT • Birth BCG for babies in Asian and other immigrant families .with high TB rates and those in contact with active respiratory tuberculosis • 2 months Polio + diphtheria /tetanus/ pertussis (DTP) + Haemophilus influenzae B (Hib) • 3 months Polio + DTP + Hib • 4 months Polio + DTP + Hib • 12-15 months Measles, mumps and rubella (MMR) PRE-SCHOOL • 3-5 years Booster polio + diphtheria/tetanus (DT) + MMR 3 years after primary course SECONDARY SCHOOL • 10-14 years BCG after tuberculin skin test SCHOOL LEAVING • 15-19 years Polio + tetanus/diphtheria (Td) MMR if not received previously
Panhypogamma-globuliriaemia This presents as recurrent sinopulmonary infection, recurrent otitis media, bronchiectasis or giardiasis infection. It may be 'early,onset' in the first two years, which is almost always the X-linked disorderdescribed by Bruton, or 'late onset' where the presentation is more variable and the inheritance pattern less certain. Failure to thrive, gastrointestinal disorders and autoimmune disorders may complicatethe clinical course. Gamma globulin replacement therapy often results in a dramatic improvement.
Selective IgA deficiency This presents with recurrent upper and lower respiratory, and gastrointestinal tract infections. Low serum IgA levels are found inbetween 1 in 400 and 700 children, but the deficiency disorders only occur in around 1 in 15 000,: this subgroup having associatedabnormalities in IgG production. They too benefit-from gamma globulin administration.
T-cell deficiencies These conditions present with frequent and severe infections with herpes simplex, measles, varicella, cytomegalovirus, Pneumocystis and fungi such as nocardia, Candida and aspergillus. T-cell deficiencies may be isolated or part of extensive immunodeficiency states in which humoral immunity is also impaired. Di George syndrome is an example of T-cell deficiency associated with congenital absence of the thymus. T-cell function is defective in Wiskott-Aldrich syndrome, ataxia telangiectasia and chronic mucocutaneous candidiasis. Bone marrow transplantation may be used to replace T-cell deficiencies, although it is of high risk especially in patients with a strong previous history of recurrent infections.
Severe combined immune deficiency This presents with failure to thrive in the first year of life, • recurrent sinopulmonary infection, • persistent candidiasis, • Pneumocystis infections, • persistent diarrhea, • severe recurrent systemic infections • disseminated viral infections. It is a rare condition and is inherited as autosomal recessive or X-linked. First cases in families are difficult to diagnose and almost, always have established infection. A low lymphocyte count (<2.8xl0*9) is an important clue worthy of further investigation. Subsequent pregnancies may be offered antenatal diagnosis and immediate postnatal investigation. Deficiency of adenine deaminase (ADA) or purine nucleoside phosphorylase (PNP) are found in certain subtypes. For children with severe combined immune deficiency (SCID) successful treatment depends upon the presence of an HLA matched bone marrow donor.
Complement (C 5,6,7 and 8) deficiencies In general deficiencies do not normally present with recurrent infections but are found as a result of investigation of the immune system for other disorders, for example vasculitis. Recurrent neisseria infections can be a presenting feature because of the specific need for components of complement to clear-this group of organisms.
Chronic granulomatous disease This presents as recurrent staphylococcal infections with abscesses in and around liver, lungs and bones, or. infection with uncommon organisms, or chronic lymphadenopathy and hepatosplenomegaly. Chronic granulomatous disease (CGD) is an X-Iinked disease in which phagocytes can ingest pathogens but are unable to mount the oxidative burst of intracellular metabolism necessary to kill them. It used to be fatal but continuous administration of antibacterial agents like trimethoprim together with vigorous antibiotic therapy for each new infection has improved the outlook in children diagnosed early and monitored closely.
Acquired immunodeficiency syndrome (AIDS) AIDS is caused by human immunodeficiency virus (HIV) of type 1 (HIV-1). HIV-1 infects CD4+ T-lymphocytes predominantly. Depletion of CD4+ lymphocytes results in immunodeficiency. The clinical picture of AIDS is the final phase of HIV infection and its manifestation, with a wide spectrum of clinical disorders. The majority of them is nonspecific.
Persisting generalized lymphadenopathy Persisting hepatomegaly Persisting splenomegaly Persisting diarrhea One or more nodes have size more than 1 cm and exist longer uian 1 month (especially substantial is enlargement of auxiliary lymph nodes) Enlargement of the liver, registered for 3 months and more Enlargement of the spleen, registered for 3 months and more Stool is three times a day for more than 1 month Clinical manifestations of HIV infection in children
Fever Persisting enlargement of salivary glands Thrombocytopenia Serious bacterial infections t = 38 CC for 4 weeks and more, 2 and more episodes of fever of obscure nature For 3 months and more Amount of thrombocytes is less than 100 000 per ml twice and more times 2 and more episodes of exacerbation or chronization of an infection (for more than 3 days in spite of the treatment) Clinical manifestations of HIV infection in children
Retardation of development Persisting or recurring oral candidiasis Cardiomyopathy Nephropathy Progressing hypotrophy, encephalopathy It lasts for 2 months and more or relapses after the course of treatment Signs of heart insufficiency Nephrotic syndrome (proteinuria, hypoalbuminemia) Clinical manifestations of HIV infection in children
CARE OF A CHILD WITH IMMUNODEFICIENT CONDITIONS A report of certain communicable diseases must be filed with the city health department upon the admission of the child. Personnel giving direct care to the child with a communicable disease should seek protection when immunization measures are; available. Frequent handwashing is essential. Isolation Gowns When isolation gowns are used, a fresh gown should be used for each patient contact. Organization of activities is essential for the economical use of supplies.
CARE OF A CHILD WITH IMMUNODEFICIENT CONDITIONS Isolation Masks If a mask is used, it should cover both the nose and the mouth, be worn no longer than 30 minutes, and be discarded immediately after use. Disposal of Wastes Paper bags for the disposal of tissues should be available within the unit. All contaminated waste should be wrapped securely and discarded in a special receptacle marked "isolation." Bedpans may be emptied into the community sewage system, using the bedpan flusher. The flusher should be handled with paper barriers. Waste cans should be lined with paper and kept covered. All reusable equipment should be cleaned, wrapped, labeled "isolation," and sterilized before routine reprocessing. Infusion bottles should be discarded after use
CARE OF A CHILD WITH IMMUNODEFICIENT CONDITIONS Care of Dishes Disposable dishes maybe requested through the dietary department. If regular dishes are used, they should be returned to the kitchen for processing in the dishwashing machine. Formula bottles should be washed and returned to the reception area of the formula kitchen.