Download
1 / 55
610 likes | 869 Views
OXYGEN THERAPY. Dr. S.Parthasarathy MD, DA, DNB., Dip.,Diab., Dip. Software based statistics. PhD (physio) Mahatma Gandhi medical college and research institute , puducherry – India painfreepartha@gmail.com. After food-- 0xygen flow is. DEFINITION.

E N D
OXYGEN THERAPY • Dr. S.Parthasarathy • MD, DA, DNB., Dip.,Diab., Dip. Software based statistics. PhD (physio) • Mahatma Gandhi medical college and research institute , puducherry – India • painfreepartha@gmail.com
DEFINITION • Oxygen therapy is the administration of oxygen at concentrations greater than ambient air (i.e. >21 %) with the intent of correction or prevention of hypoxemia
INDICATIONS • Patients with documented hypoxemia. • PaO2 < 60 mm Hg or SaO2 < 90 % in subjects breathing room air. • PaO2 less than acceptable for that specific clinical situation. • An acute care situation in which hypoxemia is suspected. It should be substantiated within a reasonable period of time
INDICATIONS • Severe trauma. • Acute myocardial infarction. • Post anaesthesia period. Supplemental oxygen is to be administered to all patients during emergence to prevent tissue hypoxia. Some factors favour prolonged therapy.
Factors Patient factors • Cardio respiratory disease. • Obesity • Elderly • Shivering Surgical factors. • Upper abdominal surgeries. • Thoracic surgeries
Pathophysiological factors. • Hypovolumia • Hypotension. • Anaemia. Analgesia factors. • Patient controlled analgesia. • IV opioid infusion. • Epidural opioids
REGARDING OXYGEN THERAPY • Hypoxic hypoxia (PaO2 is low.) very useful Anaemic hypoxia. (Anaemia. PaO2 normal.) Stagnant hypoxia. (circulatory shock) may be useful • Cytotoxic hypoxia. (cyanide poisoning) • not useful
Hypoxemia- clinical clues • Pulmonary: tachypnea, dyspnea • CVS: tachycardia, hypertension, dysryhthmias, palpitation • Haemotology: anaemia. • CNS: restlessness, disorientation, coma, paraesthesia. • Others : cyanosis, clubbing, nausea, vomiting • What is the inference ??
1000 ml o2 supplied • 250 ml consumed • 750 ml returned • SvO2 75% • Oxygen flux = CARDIAC OUTPUT × 1.34 × Hb × SATURATION
Suppose in pneumonia there is hypoxemia what are we doing by giving oxygen ?? • See next !!
Why to give? • Relieve hypoxemia. • Prevent hypoxemia. • Reduce the work of breathing. • Decrease the work of myocardium. • Improve exercise tolerance. • It is for us to see that the right patient receives the right amount of oxygen for the right length of time
FDO2 and FiO2 • FDO2 -fractional percentage of delivered oxygen by the oxygen delivery device. • FiO2 -fractional percentage of oxygen in the inspiratory air of patients. • In simple words the device may give 100% O2 but the patient may breathe 24 % O2. why?
1.The device itself • Device Oxygen flow FiO2 • Nasal catheter 2 l/min 0.28 • Transtracheal 2 l/min 0.4 catheter
2.Oxygen flow • 3.Patients inspiratory flow. • 4. Minute ventilation • 5. The mouth breathers
The oxygen delivery devices can be categorized as • Low flow systems. • Reservoir systems. • High flow systems. • Enclosure systems.
a short break • An executive rang up the doctor to say ‘ My wife has abdominal pain’. • The doctor asker her to come and examined to detect appendicitis. she was operated and went home fine. • Six months later the phone from same executive ‘ My wife has got appenticitis.’ The doctor angrily said ‘A man can have one appendix’
Variable performance devices (Low flow systems) • devices which supply oxygen at flow rates lower than the patients’ inspiratory demands. • Varying amounts of room air added to provide inspiratory volume. • Deliver FiO2 ranging from 0.22- 0.6 depending on patients’ inspiratory flow, tidal volume and oxygen flow. E.g. 1. Nasal cannula. 2.Transtracheal catheter. 3. Simple mask.4. Partial rebreathing masks. 5. Nonrebreathing masks.
Fixed performance devices (high flow systems) • provide oxygen at flow rates high enough to satisfy patients’ inspiratory demands. Such high flows (i.e. 35-40 litres approx.) are possible by • Entrainment of room air. • High flow rates and reservoirs. E.g. Venturi masks. Incubators. Tents. Hoods.
Both systems can deliver a wide range of FiO2. • It is a misconception that low flow systems deliver low FiO2 and high flow systems deliver high FiO2. • DO NOT CONFUSE LOW FLOW AND HIGH FLOW WITH LOW FiO2 AND HIGH FiO2.
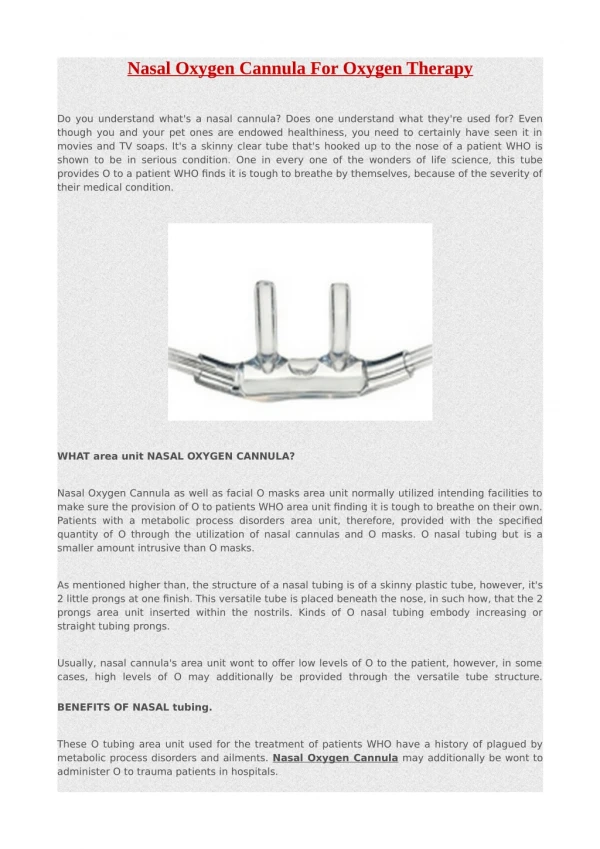
Nasal cannula • The two soft prongs are inserted into nares.The tubing is secured to the patients’ face. • FiO2 0.22-0.4 • ADVANTAGES • Simple, well tolerated, • Nonclaustrophobic. • Available for infants also. Feeding • mobility better. • Humidification not required.
Transtracheal cath.- home O2 • In hospital sterile surgical percutaneous transtracheal insertion of a stent followed by a suitable catheter a week later. • Improved compliance • cosmetic appearance. • Reduced cost of oxygen • no nasal irritation.
Simple mask • A plastic reservoir designed to fit over the nose and mouth. Internal capacity of the mask is reservoir. Holes on each side of the mask serve both as exhalation and room air entrainment ports. • ADVANTAGES : • High FiO2. • Interim therapy. • Better humidification
Problems – simple mask • High flow (5-6 l/min) necessary. • Variable performance device. • Speaking, eating difficult. • Potential for aspiration. • Co2 rebreathing possible. • Ideal for short periods
Partial rebreathing mask • FiO2 of 0.4-0.6 • Child and adult sizes √ • Better humidification. • Simple. • Useful in distress for high humidified FiO2. • High flow (6-10 l/min) necessary. • Variable performance device. • Speaking, eating difficult. • Potential for aspiration. • Uncomfortable for extended period
Nonrebreathing mask Similar to partial rebreathing mask but attached with one or two one way valves in the side of the mask. Total non rebreathing and 100% FiO2 is difficult to achieve because of face leaks and small reservoir bags
High flow systems.Air entrainment mask(venturi)FiO2 – 0.24-0.5 • Oxygen forced through a jet orifice entering the mask. As there is a pressure drop across jet orifice room air entrainment occurs through side ports. (venturi effect.) • High flows. • Fixed FiO2.
Should not be like this! No extra length tube
beware! • The performance of venturi mask may be altered by obstruction distal to the orifice resulting in higher FiO2 and lower total flows. • The performance - altered by blocks of entrainment ports. • Obstruction of the device by coughed out secretions and the altered delivery of FiO2 should be borne in mind.
High flow aerosol • Oxygen forced through a jet orifice entrains both room air and gets humidified from a bottle of water. The output is given through a Brigg’s adapter. • High flows • Fixed FiO2. • Noise. • At a higher FiO2, (>0.8) the flow may decrease to 15-20 litres /min.Hence in dyspnoeic patients needing high FiO2, it may be less useful.
Oxygen hoods - transparent enclosures designed to surround the head of an infant. • continuous humidified oxygen supplied to hood. • short term use in active infants. • A minimum flow of >7 litres - necessary. • continuous oxygen analysis and alarm systems required for safe use.
Oxygen tents -- electrically powered appliances that incorporate an air circulation system and provide temperature control. The nebulizer is connected to a transparent canopy placed over the patient. distinct fire hazard with the tent.
Supplemental oxygen is a relatively benign drug. • Before going to the possible hazards, it is to be mentioned that many patients die of hypoxia than due to potential complications of oxygen therapy
Physiological: • Beware-- preterm infants. PaO2 of more than 80 torr may be linked to retinopathy. • may cause imbalance in systemic and pulmonary blood flows in certain congenital heart diseases. • may induce pulmonary fibrosis in patients of paraquat poisoning and bleomycin intake.
Hazards • may cause CO2 narcosis in patients with COPD if the hypoxic respiratory drive is suppressed. • Inappropriate therapy ---hypoxia or hyperoxia. • Persistent high FiO2 (>60%) can induce lung damage to produce a clinical ARDS picture. • Physical. • Oxygen delivery devices can malfunction to deliver insufficient oxygen. • The devices may physically cause injuries to the face, lips nasopharynx etc.
Others. • Fire hazard is increased with oxygen therapy. • Bacterial contamination is associated with humidification systems. • Sometimes water in the humidifier may be there for years. • Dry gases can cause airway irritation.
FACTORS THAT DETERMINE WHICH SYSTEM TO START, USE, **PATIENT COMFORT. ** THE LEVEL OF FIO2 ** DISTRESSED OR NORMAL **REQUIREMENT CAN BE CONTROLLED WITHIN A CERTAIN RANGE. **THE LEVEL OF HUMIDIFICATION AND OR NEBULIZATION START—MONITOR—CHANGE--STABILIZE
A case of acute asthma comes with respiratory distress. These patients are hypoxemic and have rapid respiratory rates. • If there is no CO2 retention, venturi masks with humidification or aerosol nebulizers are useful to start with FiO2 of 0.4- 0.5. • Dry gases can be irritant to increase spasm.
2. A case of pneumothorax with respiratory distress. • These patients may need 100% O2 to wash off nitrogen (Case of air in body cavities). • patient is in distress so ideal to give 100% O2 with a Gas Injection Nebulization (GIN) because it can give high flows to meet patient demands. • A case of pneumothorax without much distress, a nonrebreathing mask to give 100% O2 is enough
3.A routine postoperative laparotomy patient. • These patients may need supplemental O2 through a venturi mask or a nasal cannula. FiO2 of 0.3 is usually enough. 4. A routine myocardial infarction patient • A nasal cannula or catheter is started with FiO2 of 0.3.This will not hinder talking or drinking by the patient as opposed to masks.
5. A case of faciomaxillary trauma with hypoxemia. • A partial rebreathing mask with FiO2 0f 0.6 is ideal. Nasal cannula or catheter is contraindicated in faciomaxillary trauma. 6. An infant with croup. • An oxygen hood with supply of humidified Fio2 of 0.4 is to be set up. Mobility of the infant may displace the hood and should be taken care of.