Download
1 / 40
450 likes | 808 Views
Clostridium difficile. BATAM bijeenkomst 17 mei 2013 Dr DJ Bac , MDL-arts Dr MA Schouten, arts-microbioloog. CDI. Berucht vanwege ribotype 027 Diverse uitbraken sinds 2000 Toename morbiditeit + mortaliteit + kosten. CDI. Clostridium difficile. Gram positieve anaerobe staaf

E N D
Clostridiumdifficile BATAM bijeenkomst 17 mei 2013 Dr DJ Bac, MDL-arts DrMA Schouten, arts-microbioloog
CDI • Berucht vanwege ribotype 027 • Diverse uitbraken sinds 2000 • Toename morbiditeit + mortaliteit + kosten
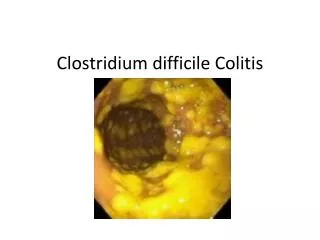
Clostridiumdifficile • Gram positieve anaerobe staaf • Produceert sporen • Produceert toxines • Nr 1 oorzaak nosocomiale diarree
Risk factors clostridium difficile • Ziekenhuisopname • Antibiotica: • > 65 jaar • IBD • PPI ?? • sondevoeding • diverticulose • chemotherapie • (GI) chirurgie • dialyse
Epidemiologie clostridium difficile Drager • Gezonde personen ~3% • Ziekenhuis ~20% • Jonge kinderen tot 80% Diarree • Hospital-acquired: ~ 10 % • Community-acquired: ~ 1,5-2 %
1elijns probleem? • Clostridiumdifficileinfection: it’s a familyaffairUK 2007-2012: 238 patiënten met CDI; verspreiding na ontslag? slechts in 3 gevallen verspreiding thuis (1) • Community-associatedClostridiumdifficileinfection: Howreal is it? (2)Studie CDC: CA= diarree niet voorafgegaan door ziekenhuis bezoek afgelopen 3 maanden, >10.000 gevallen; 32% CA: hiervan 25% opgenomen na vaststellen CDI, recurrencerate 9%, PFGE type NAP1, NAP11, NAP4Risicofactoren CA CDI: AB gebruik, protonpomp remmersliteratuur: vlees, huisgenoten met CDI, kinderen < 2 jaar. 1: ICHE 2013, 2: Anaerobe 2013
1elijns probleem? • Clostridiumdifficilecarriage in healthyinfants in the communityasymptomatischdragerschap volwassenen 1-7%Kinderen tot 2 jaar 2-75% drager maar zelf zelden ziekStudie: 10 gezonde kinderen van 1 jaar gevolgd + screening 2 dagopvangcentraAlle 10 verwerven CD en bleven maanden POSDagverblijf 45% van de 85 kinderen CD POSRisicofactoren: ab gebruik, gebruik ab moeder zwangerschap, verandering voeding (met name bij verdwijnen Bifidobacteriumcave melk / BV minder CD, flesvoeding meer CD)Geen relatie met aantal siblings of dierenRecente ziekenhuis opname enige risicofactor voor kolonisatie pathogene stam CID 2012
1elijns probleem? • Clostridiumdifficilecontamination of public tap water distribution system during a waterborneoutbreak in Finland • Nov-dec 2007 drinkwater Nokia gecontamineerd met rioolwater • Grote uitbraak gastro-enteritis; Rol Clostridiumdifficile ?10.000 inwoners, 8000 ziek, 1000 behandeld, 17 CD POS (65 getest) • 12 CD isolaten gevonden in water (5 kraanwater, 7 riool) • Aantal malen zelfde stam in water en patiënt SAGE 2013
Dieren • Clostridiumdifficileinfection in the community: a zoonoticdisease? (1) • Review LUMC; CD komt zowel bij mensen als dieren voor; verschillende biotypes • Bij vinden nieuwe types als verwekker humane infecties dan zoeken naar dierlijk reservoir • Clostridiumdifficilein faecesfromhealthydogs and dogswithdiarrhea (2) • Stockholm; 50 gezonde honden: 2 met CD; niet toxine producerend20 honden met diarree: 2 met CD; toxine producerend, humane types 1: CMID 2012, 2: AVS 2013
Voeding • Detection of Clostridiumdifficilein retailgroundmeatproducts in Manitoba • 48 porties vlees (rund en varken); 6,3% CD POS • Verschillende types; wel allemaal bekend humane toxine producerende stamen JIDM 2012
Diagnostiek • Gold standard: cytotoxicity assay • Kweek met toxinebepaling • Elisa (toxin A and or B, or GDH) • 72-92 % sensitiviteit • 89-98 % specificiteit • PCR • Sensitiviteit 92% • Specificiteit 96% • Sigmoidoscopy
Behandeling • De beste behandeling is nog steeds preventie! • Lokaal: antibioticum formularium ZGV • Gebaseerd op SWAB richtlijn • SWAB weer gebaseerd op ESCMID
“Infection control” strategie Kelly & Lamont. NEJM 2008;359:1932–40 Vonberg et al ClinMicrobiol Infect 2008;14(Suppl. 5):2–20
Behandeling: ESCMID recommendations:An initial mild episode of CDI • Discontinuation of the antibacterial treatment that induced CDI, if possible • Avoidance of treatments that reduce gut transit • e.g. opioids, including those used in diarrhoea relief (loperamide etc) • Provision of supportive care • e.g. fluid and electrolyte replacement • Observation for signs of clinical deterioration Bauer et al. ClinMicrobiol Infect 2009;15:1067–79.
Behandeling: ESCMID recommendations:First episode of CDI • Aim of treatment is to eradicate C. difficilefrom the intestines and promote restoration of the normal colonic microflora • Cessation of antibacterial therapy, if possible, is usually the first step * Intravenous (IV ) if oral therapy is not possible Bauer et al. ClinMicrobiol Infect 2009;15:1067–79.
Metronidazol 3 dd 500 eerste keus: po en iv geen selectie VRE Goedkoop vaak recidieven Behandeling (10-14 dgn) • Vancomycine • 4 dd 125-500 mg • tweede keus: • alleen po • selectie VRE • Duur • vaak recidieven Ernstige colitis vancomycin
Snapshot of current treatments for initial episodes of CDI in Europe Treatments used in an initial episode of CDI in a recent European survey Bauer et al. Lancet 2011;377:63–73.
Cure rates: Metronidazole & vancomycin p=0.02 p=0.36 p=0.006 39/40 69/71 30/31 37/41 66/79 28/38 *Patients were stratified by mild or severe disease based on severity assessment score developed for this study. Patients received one point each for age >60 years, temperature >38.3°C, albumin level <2.5 mg/dL, or peripheral white blood cell count >15,000 cells/mm3 within 48 hours of enrolment. Two points were given for endoscopic evidence of pseudomembranous colitis or treatment in an intensive care unit. Patients with ≥2 points were considered to have severe CDI. Zar et al. Clin Infect Dis 2007;45:302–7.
Recurrence of CDI • Recurrence of CDI has been identified by ESCMID as the most important problem in the treatment of CDI1 • CDI recurrence is common, occurring in up to 32% of cases within 30 days following treatment2–4 • Rate of reported recurrences strongly depends on definition applied1 • Recurrence appears to be related to a combination of:5 • A failure to re-establish the colonic microflora • The presence in the intestines of spores of C. difficile • A sub-optimal host immune response to the infecting organism and its toxins Bauer et al. ClinMicrobiol Infect 2009;15:1067–79; Louie et al. N Engl J Med 2011;364:422–31; Lowy et al. N Engl J Med 2010;362:197–205; Bouza et al. ClinMicrobiol Infect 2008;14:S103–4; DuPont. N Engl J Med 2011;364:473–4.
Risk factors for a recurrence of CDI • Immunocompromised patients1 • Exposure to other antibacterial agents that disrupt the normal colonic microflora2–5 • Previous episode of CDI2,4–6 • Renal impairment7,8 • Aged 65 years or over2,4,9 • Impaired immune response to C. difficile toxin A2 • Severe underlying disease2 • Prolonged hospitalisation9 • Concomitant use of antacid medications (PPI)10 • Intensive care unit (ICU) stay5 PPI, proton pump inhibitor McFarland et al. Am J Gastroenterol 2002;97:1769–75; Do et al. Clin Infect Dis 1998;26:954–9; Bauer et al. ClinMicrobiol Infect 2011;17(Suppl 4):A1–A4; Pépin et al. Clin Infect Dis 2005;40:1591–7; Kwok et al. Am J Gastroenterol 2012;107:1011–9. Cohen. J PedGastroenterolNutr 2009;48:63–5; Kyne et al. Lancet 2001;357:189–93; Bauer et al. ClinMicrobiol Infect 2009;15:1067–79; Bauer et al. Lancet 2011;377:63–73; Hu et al. Gastroenterology 2009;136:1206–14;
Pharmacotherapy of CDI: First recurrence • ESCMID recommends treating a first recurrence as a first episode unless the disease has progressed from non-severe to severe *Intravenous (IV ) if oral therapy is not possible; tid, three times daily; qid, four times daily Bauer et al. ClinMicrobiol Infect 2009;15:1067–79.
ESCMID recommendations: Second and later recurrences • ESCMID recommends treating second or later recurrences in the same way as severe first recurrence • With the option of using tapered or pulsed dosing regimens Bauer et al. ClinMicrobiol Infect 2009;15:1067–79.
ESCMID recommendations:Surgical intervention • In the minority (<5%) of patients who develop fulminant colitis, surgical intervention (colectomy) may be needed • Surgical intervention carries a high rate of mortality • Optimal timing for colectomy has not been established • Current guidelines recommend intervention before: • The disease becomes too severe • Serum lactate levels exceed 5 mmol/L Bauer et al. ClinMicrobiol Infect 2009;15:1067–79.
Clinical limitations associated with current treatments for CDI • Although metronidazole and vancomycin are effective in a first episode of CDI, therapy remains suboptimal • Among the most significant drawbacks of current therapy for CDI are: • Rates of treatment failure with metronidazole of up to 18%1 • Rates of recurrent infection following treatment with metronidazole and vancomycin of up to 32% within 30 days following treatment2–4 • Risk of overgrowth of vancomycin-resistant enterococci(VRE) in patients who are already colonised with VRE5 Aslam et al. Lancet Infect Dis 2005;5:549–57; Louie et al. N Engl J Med 2011;364:422–31; Lowy et al. N Engl J Med 2010;362:197–205; Bouza et al. ClinMicrobiol Infect 2008;14:S103–4; Al-Nassir et al. Antimicrob Agents Chemother 2008;52:2403–6.
Fidaxomicine • Macrocyclisch antibioticum • Remt bacteriële RNA polymerase • Smal spectrum; Gram negatieve bacteriën resistent • Remt sporenvorming • Remt toxine productie • Wordt beperkt geresorbeerd: lokaal werkzaam • Zwangerschap / lactatie: onbekend • Bijwerkingen: misselijkheid, braken, obstipatie... • Dosering 2 dd 200mg 10 dagen
Fidaxomicine • Extramuraal vergoed via GVS mits 18 jaar of ouder CDI Recidief na metronidazol behandeling Ernstige infectie • 1620 euro per kuur