Download
1 / 83
860 likes | 1.08k Views
Q. L. Endocrine & Liver Diseases. The Pathological Basis of Disease - Graduate Studies Course CMM 5001. Qiao Li, MD, PhD Dept of Pathology & Laboratory Medicine Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Ext. 8491. Q. L. Outline. Adrenal Gland

E N D
Q L Endocrine & Liver Diseases The Pathological Basis of Disease - Graduate Studies Course CMM 5001 Qiao Li, MD, PhD Dept of Pathology & Laboratory Medicine Faculty of Medicine University of Ottawa qiaoli@uottawa.ca Ext. 8491
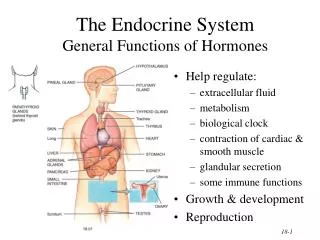
Q L Outline • Adrenal Gland • Anatomy Histology & Function • Steroid Hormones • Cushing Syndrome • Clinical Case Presentation • Liver • Anatomy, Histology & Function • Metabolic & Toxic Conditions • Cirrhosis • Tumors • Clinical Case Presentation
Q L Adrenal Gland • Anatomy, Histology & Function • Steroid Hormones • Cushing’s Syndrome • Clinical Case Presentation
Adrenal Gland – Low Power Medulla Zona fasciculata Capsule Zona reticularis Zona glomerulosa Periadrenal fat
Q L Adrenal Gland • Anatomy, Histology & Function • Steroid Hormones • Cushing’s Syndrome • Clinical Case Presentation
Q L Adrenal Cortex Steroids Zone Class Representative Physiologic Effects glomerulosaMineralocorticoids Aldosterone salt and water homeostasis fasiculataGlucocorticoids Cortisol carbohydrate metabolism reticularisSex Steroids Androgens minimal effects
Histone acetylation p300/CBP TAFII250 GR GR TBP RNA Pol II Q L Glucocorticoids & the Receptor • Cortisol, the majority of glucocorticoid activity in most mammals, also known as hydrocortisone. • About 90% of circulating cortisol binds to plasma proteins, corticosteroid-binding globulin (transcortin), decreasing the rate of metabolic clearance and the concentration fluctuation (the transcortin bound cortisol is biologically inactive). • Nobel Prize, Edward Kendall, Tadeus Reichstein & Philip Showalter Hench
CRH Q L Control of Cortisol Secretion HPA Axis Hypothalamus Pituitary ACTH Cortisol Adrenal Cortex Dr. Gary Farr
Q L Adrenal Gland • Anatomy, Histology & Function • Steroid Hormones • Cushing’s Syndrome • Clinical Case Presentation
CRH ACTH Cortisol Q L Cushing’s Syndrome • Excessive Endogenous Cortisol • - ACTH independent: cortical tumor • - ACTH dependent: pituitary adenoma • small cell carcinoma • Administration of Glucocorticoids • - The most common cause • Clinical Manifestations • weight gain, truncal obesity and moon face • - muscle weakness, thin arms and legs • hypertension and osteoprosis • moodiness, irritability, or depression Harvey Cushing 1912
Q L Adrenal Gland • Anatomy, Histology & Function • Steroid Hormones • Cushing’s Syndrome • Clinical Case Presentation
History • A 35-year-old female with weakness, mainly of the shoulders and thighs, increasing thirst, headache, easy bruisibility and depression. • Physical examination: moon face, truncal obesity, purple striae on the lateral aspects of abdomen, reduced strength in the proximal muscles of both shoulders and hips. • Blood pressure: 180/110 • The patient was then admitted to the hospital and underwent various laboratory test.
Laboratory Test Plasma glucose: 300 mg/dL (normal 70-110 mg/dL) Overnight DEX suppression plasma cortisol: 10 µg/dL next 9 am (normal < 5 µg/dL) Plasma cortisol: 28 µg/dL at 9 am (normal 10-25) 25 µg/dL at 6 pm (normal < 10 µg/dL) 24-hour urine free cortisol: 200 µg/day (normal < 50 µg/day) Plasma ACTH: 125 pg/mL (normal 20-100 pg/mL) Low-dose DEX suppression (0.5 mg/6 hours for 48 hours, 2 mg/day): urinary 17-hydroxycorticosteroids, 12 mg/day (normal < 4 mg/day) High-dose DEX suppression (2 mg/6 hours for 48 hours, 8 mg/day): urinary 17-hydroxycorticosteroids, 3.6 mg/day (suppressed by 70%) Proceed to MRI & CT scanning of the brain and adrenal glands Hall mark: loss of circadian hormone rhythm
Adrenal Glands – Gr / CS Nodular Cortical Hyperplasia Confluent Nodules
Adrenal Glands – Gr / CS Nodular Cortical Hyperplasia Confluent Nodules
Adrenal Glands – Low Power Nodular Cortical Hyperplasia Nodule
Adrenal Glands – Low Power Nodular Cortical Hyperplasia Nodule
Adrenal Glands – High Power Nodular Cortical Hyperplasia
Q L Diagnosis Cushing’s Syndrome
Q L Liver • Anatomy, Histology & Function • Metabolic & Toxic Conditions • Cirrhosis • Tumors • Clinical Case Presentation
Liver - Anatomy Columbia University Howard J. Worman, M. D.
Liver - Gross Columbia University Howard J. Worman, M. D.
Liver - Cut Surface Portal vein Hepatic vein Columbia University Howard J. Worman, M. D.
Q L Function of the Liver, hepatocyte Metabolism - Dietary carbohydrates, protein and fat Synthesis - Albumin, clotting factors & complement proteins Storage - Glycogen, triglycerides, vitamins & minerals Detoxification - Endogenous substances & foreign compounds Production - Bile for fat digestion & waste elimination
Liver – Histology Portal triads Zoning by oxygen supply Central vein Columbia University Howard J. Worman, M. D.
Q L Liver • Anatomy, Histology & Function • Metabolic & Toxic Conditions • Cirrhosis • Tumors • Clinical Case Presentation
Q L Pathophysiology Alcohol: absorbed from the stomach and small intestine metabolized through oxidation in liver Acetaldehyde by alcohol dehydrogenase & cytochrome P‑450 2E1 Acetate by mitochondrial acetaldehyde dehydrogenase.
Q L Alcoholic Liver Disease • Excess alcohol ingestion • the most common cause of liver disease • Risk for severe hepatic injury • daily intake > 40 or 80 g alcohol for 10 years • Individual susceptibility • females > males • body mass • genetic background
Liver, Alcoholic Hepatic Steatosis (Fatty Liver) – Gr / CS Columbia University Howard J. Worman, M. D.
Liver, Alcoholic Hepatic Steatosis (Fatty Liver) - Histology Columbia University Howard J. Worman, M. D.
Liver, Alcoholic Hepatic Steatosis (Fatty Liver) – High Power Columbia University Howard J. Worman, M. D.
Liver, Alcoholic Hepatitis - LP Trichrome stain
Liver, Alcoholic Hepatitis - LP Trichrome stain
Liver, Alcoholic Hepatitis - MP Mallory bodies Hepatocytes
Liver, Alcoholic Hepatitis - MP Mallory bodies
Liver, Alcoholic Hepatitis - MP Hepatocytes
Liver, Alcoholic Cirrhosis – Gross Columbia University Howard J. Worman, M. D.
Liver, Alcoholic Cirrhosis – MRI Enlarged spleen Columbia University Howard J. Worman, M. D.
Liver, Alcoholic Cirrhosis – MRI Enlarged spleen Columbia University Howard J. Worman, M. D.
Liver, Alcoholic Cirrhosis – Gross Columbia University Howard J. Worman, M. D.
Liver, Alcoholic Cirrhosis – CT Enlarged spleen Columbia University Howard J. Worman, M. D.
Liver, Alcoholic Cirrhosis – CT Enlarged spleen Columbia University Howard J. Worman, M. D.
Liver, Alcoholic Cirrhosis - CS Regenerative Nodules