Download

1 / 0
0 likes | 102 Views
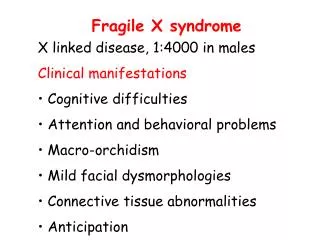
6. Discuss the genetics of Fragile X syndrome with special emphasis on the molecular basis of the disease. Trinucleotide Repeat Disorders Friday 4 th September 2009. Stacey Sandell. Fragile X syndrome. Fragile X syndrome is one of the most common forms of inherited mental retardation.

E N D