Download
1 / 28
290 likes | 300 Views
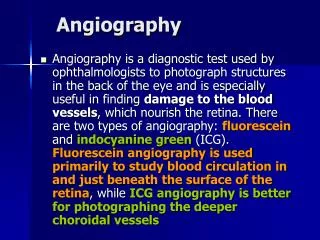
IST3 Perfusion and Angiography Study. Collaborators Meeting ESC 2010, Barcelona, May 27 th 2010. Background. Perfusion and angiography imaging used increasingly in acute stroke Radiation dose Problems with renal function and diabetes Delays treatment

E N D
IST3 Perfusion and Angiography Study Collaborators Meeting ESC 2010, Barcelona, May 27th 2010
Background • Perfusion and angiography imaging used increasingly in acute stroke • Radiation dose • Problems with renal function and diabetes • Delays treatment • Wide variation in terminology and definitions • Uncertainty about processing and interpretation
CT radiation exposure NEJM 2009;361:849-57 : Survey of952,420 adults, USA: Mean 2.4 mSv 1 CT brain scan per year Medium to high doses in 2% and 0.2% respectively (ie at or above max permitted for radiation worker) New York Times 15th Oct 2009 Cedars-Sinai Medical Center, …… had mistakenly given up to eight times the normal radiation dose to 206 possible strokevictims ..involved CT brain perfusion scans. Cedars-Sinai began investigating the procedure in August after a patient noted a “temporary patchy hair loss.”
Radiation Doses: CT, CT angiography, CT perfusion Procedure Dose background (mSv) radiation equiv. (years) CT brain 1.8 1.0 CT angio 2.2 1.5-2.0 CT perfusion 3-5 1.5-2.5 2x CT, CTA, CTP 22 9 Better evidence required to show that benefits outweigh risks, costs, time
Aims 1. Do acute ischaemic stroke patients with imagevidence of tissue at risk (mismatch) on either CT with CTP or MR DWI/PWI, have a) less infarct growth and b) better functional outcome if treated with rt-PA than do patients without mismatch? 2. Which perfusion parameter (CBF, CBV, MTT or some derivative), processing method (qualitative, quantitative) and threshold best predicts: a) infarct growth at 24 hours and b) poor functional outcome at six months? 3. Can we clarify imaging features on plain CT or MR DWI that differentiate viable from non-viable tissue?
Progress • Funding NIHR EME 2009-2012 • Protocol • Image acquisition guidance • Image processing established + piloted • Recruitment • Questions to be resolved
Imaging Parameters • Guide Line Perfusion Acquisition Parameters • Based on experience in current studies • Compatible with STIR recommendation • Acute Stroke Imaging Research Roadmap. Stroke, 2008; 39: 1621 – 1628 • 3 key points – CT perfusion • 80 kvp for the perfusion • Start Imaging soon enough • Be careful of delay time between injection and acquisition • Image for long enough • Capture full signal time curve - CT – non contrast whole brain volume needed – please send as well
Imaging Parameters – rationale and common errors • Delay required to reduce dose • At least 1 pre-contrast volume • Must capture washout in white matter and infarct to construct adequate signal-time curve • Commonest errors: • To long a delay between contrast and acquisition • Not imaging for long enough
Data processing • Datasets submitted by normal IST3 routes • Guideline acquisition parameters available • Please remember to submit CT volume scan as well • Perfusion and Angiography processed separately • Centralised processing • Catalogued • Quality Assured • Processed • PMA, ASIST • Analysed • Angiography read according to TIMI and MORI scores
Perfusion Analysis • Construct perfusion image • Register data sets between different time points to map lesion development • MR and CT have different resolution, field of view and slicing planes • Requires interpolation
IST-3 Perfusion and AngiographyPerfusion analysis • Qualitative visual rating of perfusion lesion • and mismatch extent • IST-3 • ASPECTS • for all perfusion parameters including raw data • 2. Quantitative tissue perfusion threshold • analysis
Benefits of registering CT and MR at different time points – tissue measurements K Rowland, T Carpenter, J Wardlaw Pre-randomisation MR DWI image
Measure tissue change in CT attenuation 20 patients, mean age 75.5 ± 12.5 years; mean admission NIHSS 14 ± 7; mean time from stroke to CT 174 mins (range 75-330). All differences ischaemic:contralateral tissue p 0.01
IST-3 Perfusion and AngiographyPerfusion Parameters to be tested
IST-3 Perfusion and AngiographyPerfusion Parameters to be tested ARE THERE ANY OTHER PARAMETERS THAT SHOULD BE TESTED???
IST-3 Perfusion and AngiographyPerfusion Parameters to be tested
IST-3 Perfusion and Angiography Study Recruitment – 12th May 2010 Strong preference for CT pre-randomisation, MR at follow up.
Target sample estimate 60% will have mismatch overall; 70% with mismatch will have infarct growth vs. 30% without mismatch; rt-PA will reduce infarct growth by 20% in those with, but not those without mismatch. Difference in infarct growth detectable, + vs - rt-PA, + vs - mismatch (80% power, alpha of 0.05): N difference in infarct growth 100 27% 160 20% 400 15% We acknowledge that, with at most 300 patients, we may not detect a “rt-PA x mismatch effect”
TARGET SAMPLE Pre-randomisation so far: • 73 perfusion • 99 angiography Rate: • Last year 0.8 per week • Current 1.2 per week Potential by mid 2011: • 150 - 200 patients, possibly as many as 300
IST3 Perfusion and Angiography Study • Ways to encourage recruitment • Encourage sending of data • Collaborator meeting
IST3 Perfusion and Angiography Study Thank you
Perfusion analysis – obstaclesCT to MR registration artefact Change of resolution (MR registered to CT)
Perfusion analysis – obstacles CT to MR registration artefact Change of slicing plane CTP registered to MRP CT volume CTP registered to MRP CT volume
Perform registration as normal Draw ROI on original image Apply transform to ROI Requires shape based interpolation Solution: ROI transformation Change of slicing plane
Down Sampling Change of resolution (MR registered to CT)
Down Sampling Change of resolution (MR registered to CT)
ROI transformation Change of slicing plane MR Registered to MRP CT MR Registered to MRP CT