Download
1 / 19
190 likes | 204 Views
TOXICITY OF NUTRIENTS. NUTRIENTS. Many food chemicals are nutrients. Nutrients are necessary for growth, maintenance and reproduction of living organisms. Macronutrients: fats, carbohydrates, and proteins Micronutrients: vitamins, minerals, trace elements.

E N D
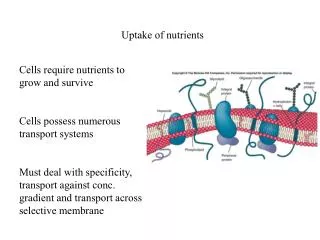
NUTRIENTS • Many food chemicals are nutrients. • Nutrients are necessary for growth, maintenance and reproduction of living organisms. • Macronutrients: fats, carbohydrates, and proteins • Micronutrients: vitamins, minerals, trace elements. • Define the intake levels as recommended dietary allowance (RDA) dietary reference intake (DRI).
Carbohydrates: adverse effect • Individuals with abnormal tolerances or intolerances (glucose, lactose). • Lactose intolerance is prevalent in populations from Far East and Middle East and Africa. • When they digest lactose, they experience gastric distress, cramping and diarrhoea. • The individuals lack the enzyme lactase to break down lactose to monosaccharides for absorption. • lactose remain in the GI tract, fermentation of lactose in the colon, producing more diarrhea and gastric problems. • Congenital defects, particularly infants.
Lipids: adverse effects Lipids and their role in chronic diseases such as heart disease and cancer. Heart disease is not a dominant factor of death, but also a primary cause of permanent disability, and reduce ability to be active. Longer hospitalization than does any other disorder. Protein: adverse effects Allergic reactions or hypersensitivity. Excessive ingestion of protein can lead to liver and kidney hypertrophy (animal study). Studies on humans have shown that ingestion of high-protein diets increases calcium excretion.
Vitamins Insufficient vitamin intakes can lead to deficiency diseases, which if left unchecked can be fatal.toxicity from vitamins can be induced from large concentrations of vitamin supplements or by misuse of specific foods. Fat-soluble vitamins Large intake of vitamin A & D can cause classical symptoms of toxicity. Excessive intake of vitamin A results in permanent liver damage and stunted growth. Usually toxic symptoms are reversed when excessive intake s are stopped. Common foods pose no problem (daily recommendation 1000 microgram/g) Can cause problem: polar bear liver, or shark, halibut, and cod liver oils (can contain up to 30,000 microgram/g).
Children can be at risk. Acute toxicity can appear in a matter of hours. Symptoms: anorexia, bulging fontanelles, hyperirritability, vomiting, headaches, dizziness, drowsiness, swelling. Chronic: take few to several months, anorexia, headache, sore muscles, bleeding lips, hair loss, cracking and peeling skins, nose bleed, liver and spleen enlargement and anemia. Excessive vitamin D intakes (from supplements and fish liver oils)resulted in a variety of toxic effects including death. Excessive ingestion: hypercalcemia, membrane damage, hypertension, cardiac insufficiency, renal failure and hyperchromic anemia. Withdrawing the vitamin can reverse the symptoms.
Children at risk (if consume 5x RDA) 20 to 20 microgram/d considered safe. Acute toxicity: symptoms include anorexia, nausea, vomiting, diarrhea, headache. Chronic: weight loss, constipation, fever, hypercacemia, and calcium deposition in soft tissues. Vitamin E and K: high doses appear to be relatively non-toxic. Some studies showed that intake of vitamin E greater than 500mg/d (50 x RDA) can impair functioning of white cells and immune system. Can antagonize vitamin’s K role in blood clotting. Vitamin K (fat soluble): readily excreted from the body. Water soluble vitamin K can lead to jaundice and hemolytic anemia.
Water soluble vitamins • As a group lower toxic effect s compared to fat soluble vitamins, they are not retained in the body. • Excess will be eliminated rapidly in the urine, but some side effects are reported: • Niacin: large therapeutic dose (100 to 300 mg or 20 mg intrvaneous) can lead to vasodilative effects. • Symptoms: flushing reaction, cramps, headache, and nausea. • High dose of niacin used to reduce serum cholesterol. • Nicotinamide do not lower serum cholesterol.
Folacin (folic acid): high dose of folic acid can mask pernicious anemia from Vitamin B12 deficiency. If go unnoticed can lead to severe neurological damage. High doses (>15mg) of folic acid are assocoated with GI disturbance, irritability, malaise, hyperexcitability, disturbed sleep and vivid dreams. Vitamin B6 (Pyridoxine):toxicity when high dose 20x the therapeutic dose, can result in convulsion disorder. Other water soluble vitamin (pantothenic acid and thiamine) show few adverse effect, not from dietary sources.
Mineral and trace elements • Depends on individuals and circumstances of exposure. • If easily stored in tissues, ingestion of lower concentration may produce toxic effect over time. • May be as a result of absorption and excretion factors, immobilization or storage of toxic element (bone storage) and detoxification mechanisms. • Magnesium: hypermagnesemia., concomitant renal failure. Neuromuscular symptoms are common.
Iron: iron overload as in hereditary hemochromatosis. Iron is absorbed in excess what is needed by the body, accumulation of non-protein bound iron and transferrin. Can result in clinical complications (diabetes mellitus, endocrine abnormalities, cardiomyopathy, arthritis, liver cirrhosis, hepatic cancer). Zinc:long term intake of 6 to 20 times the RDA can produce toxicity. Symptoms: impaired immune response, reduction in high density lipoprotein (HDL) cholesterol level, induced copper deficiency (anemia). High dose of zinc in lozenges for common cold (taken every 2 h, contain 13 mg of zinc.
Copper: toxicity occurs when the level is exceeded the capacity of the liver to bind copper. GI distress when copper intake of 5 mg/d. Weakness, listless, and anorexia are early signs. Followed by hepatic necrosis, vascular collapse, coma, and death. Manganese: oral toxicity is rare. Toxicity from airborne resulting in pancreatitis and neurological disorders. Selenium:the range between adequate selenium and toxicity is narrow 0.1 mg and 2 mg/kg of diet, respectively. Long term intake of 4 to 5 mg/kg from diet sufficient to cause growth inhibition and result in tissue damage of the liver. In human: nausea, weakness, diarrhea and eventually hair loss, changes in nails, mottling of teeth, lesions of the skin and nervous system.
Antinutrients • 3 broad classes of antinutrients: • Antiproteins • Antiminerals • Antivitamins
Antiproteins • Substances that interfere with the digestion, absorption or utilization of proteins. • Present in plants and animals. Examples: • Lactins: have binding sites for cell receptors similar to what antibodies have. • Lectins also called hemaggulutinins, can agglutinate red blood cells.
Lactins have been isolated from legumes; soybean, peanut, lima beans, kidney beans, fava beans, lentils, peas, potatoes, banana, mango and wheat germ. Lactins binds strongly to intestinal mucosa cells and interfere with amino acids, thyroxine and fat absorption; therefore such lactins are goitrogenic. Ricin from castor oil beans cause intestinal necrosis. Most lactins are inactivated by moist heat; streaming is effective. Dry heat ineffective.
Antiminerals • Substance that interfere with absorption or metabolic utilization of minerals. • Examples: phytic acid, oxalic acid, glucosinolates, dietary fiber, and gossypol. • Phytic acid affect absorption of iron. • Sources: bran and germ of many plant seeds and in grains, legumes,nuts and spices. • Form precipitate with magnesium, zinc, copper, and manganese. Reduced bioavailability of the minerals e.g formation of soy bean protein-phytate complex.
Oxalic acid: reduce availability of minerals. Sources of oxalic acid are rhubarb, spinach, beets, potatoes, tea, coffee and cocoa. Drink tea, concern with Ca deficits via complexes, counterbalanced by adding milk when drinking tea. Glucosinolate: inhibit iodine uptake into thyroid (goitrogenic). Sources: rutabaga, turnips, cabbage, peaches, strawberris good source of glucosinolates. Dietary fiber :plants cell walls that are not digested. Dietary fiber can act like ion exchangers and bind minerals. Affect calcium, magnesium, zinc and phosphorus absorption. Gossypol:phenolic compound isolated from cotton seed, chelate iron and bind amino acids.
Antivitamins • Substances that inactivate or destroy vitamins or inhibit the activity of a vitamin in a metabolic reaction and increase individual’s need for vitamins. • Diverse, not simple characterization. • E.g. ascorbic acid is oxidized by ascorbic acid oxidase, enzymes found in fruits and vegetables. • Fresh juice loses 50% of ascorbic acid in less than 1 h under aerobic conditions.
Raw fish contains thiaminase, antivitamin for thiamin. Tannins in plants destroy thiamin. Mushrooms contain vitamin B6 antagonists. Linatine in linseed oil is an antipyridoxine. Avidin (heat-sensitive compound in egg white) forms complex with biotin.