Download
1 / 46
490 likes | 772 Views
Frostbite. ا. سرمازدگي. عوامل موثر. زمان برخورد، رطوبت،باد، ارتفاع، پوشش و شرايط طبي و كلي فرد، از عوامل تأثير گذار در نوع آسيب هستند پوست تيره. علائم باليني. علائم باليني. درمان درمحل حادثه. لباسهاي خيس و چسبنده بايد خارج شوند

E N D
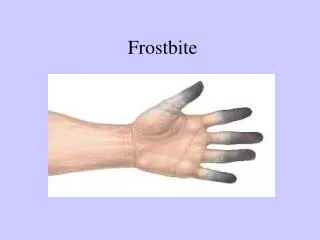
Frostbite ا سرمازدگي
عوامل موثر زمان برخورد، رطوبت،باد، ارتفاع، پوشش و شرايط طبي و كلي فرد، از عوامل تأثير گذار در نوع آسيب هستند پوست تيره
درمان درمحل حادثه لباسهاي خيس و چسبنده بايد خارج شوند اندام درگير بايد بالا برده شود و با گازهاي خشك استريل پانسمان شود انگشتها بايستي از يكديگر جدا شوند از آسيبهاي بيشتر سرما بايد جلوگيري كرد در بيشتر موارد از درمانهاي تهاجمي زخم بايد دوري كرد
گرم كردن سريع مالش برف بر روي بافت يخ زده پنی سیلین پروفیلاكتيك ايبوپروفن خوراكي
Severe hypothermia (body temperature30°C [86°F]) is associated with marked depression ofcritical body functions that may make the victim appear clinically dead during the initial assessment
Prevent additional evaporative heat loss by removing wetgarments and insulating the victim from further environmental exposures • Do not delay urgent procedures, such as intubation and insertion of vascular catheters, but perform them gently while closely monitoring cardiac rhythm. • These patients are prone to develop ventricular fibrillation (VF)
Patients in cardiac arrest will require CPR Moderate (30°C to 34°C [86°F to 93.2°F]): start CPR, attemptdefibrillation, establish IV access, give IV medications spaced at longer intervals, provide active internal rewarming that is profound enough to require CPR
Severe (30°C [86°F]): start CPR, attempt defibrillationonce, withhold medications until temperature 30°C (86°F), provide active internal rewarming
Patients with a core temperature of 34°C (93.2°F)may be passively rewarmed with warmed blankets and awarm environment
Assess the pulse to confirm cardiac arrest or profound bradycardia for 30 to 45 seconds because heart rate and breathing may be very slow
If the hypothermic victim has not yet developed cardiacarrest • If the hypothermic victim is in cardiac arrest • When the victim is hypothermic, pulse and respiratory rates may be slow or difficult to detect • warmed (42°C to 46°C [108°F to 115°F])humidified oxygen during bag-mask ventilation
But if ventricular tachycardia (VT) or VF is present, defibrillation should be attempted. • AEDs • If the patient does notrespond to 1 shock • rewarming the patient to a range of 30°C to 32°C (86°F to89.6°F) before repeating the defibrillation attempt
If coretemperature is >=30°C (86°F), successful conversion to normalsinus rhythm may not be possible until rewarming
more aggressive active core rewarming techniques • The hypothermic heart may be unresponsive to cardiovascular drugs, pacemaker stimulation, and defibrillation • IV drugs are often withheld if the victim’s core body temperature is <30°C • If the core body temperature is >30°C, IV medications may be administered but with increased intervals between doses
If the patient fails to respond to the initial defibrillation attempt or initial drug therapy, defer subsequent defibrillation attempts or additional boluses of medication until the core temperature rises above 30°C
Techniques for in-hospital controlled rewarming include administration of warmed, humidified oxygen (42°C to 46°C), warmed IV fluids (normal saline) at 43°C , peritoneal lavage with warmed fluids, pleural lavage with warm saline through chest tubes, extracorporeal blood warming with partial bypass, and cardiopulmonary bypass
Routine administration of steroids, barbiturates, and antibiotics has not been documented to increase survival rates
سندرم كمپارتمان فشار طبيعي بافتها حدود صفر و معمولاَ زير 10 ميليمتر جيوه است. جريان خون مويرگي با فشار بالاتر از 20 ميليمتر جيوه مختل ميشود در فشارهاي بالاتر از 30 تا 40 ميليمتر جيوه آسيب عضلات و اعصاب ايجاد ميشود
علائم باليني درد Pain پارستزي Pulse less درد با حركات پاسيو Pallor Paralysis
درمان درمان قطعي سندرم كمپارتمان فاشيوتومي است برش بر روي سر تا سر كمپارتمان براي كاهش فشار داده مي شود. زخم باز نگه داشته می شود فشار کمتر از 15 میلیمترجيوه ايمن است
فشار بين 20 تا 30 در صورت باقيماندن بيش از چند ساعت ممكنست سبب آسيب شود در اين موارد بايستي بيمار به دقت تحت نظر قرار گيرد و فشار مكرر اندازه گيري شود فشار 30 تا 40 ميليمتر جيوه انديكاسيون فاشيوتومي اورژانس است
رابدوميوليز سوء مصرف الكل و مواد مسموميت تروما عفونت فعاليت فيزيكي بيش از حد آسيبهاي ناشي از گرما
CK 5 برابرافزايش هیپوولمی، اسیدوز یا اسیدوری، انسداد توبولر و وجود عوامل نفروتوكسين
درمانمراقبتهاي پيش بيمارستاني در بيماران دچارآسيب له شدگی يا بيماران در معرض خطر ايجاد آن و احتمال رابدوميوليز ، و زمان خروج از محل يا انتقال طولاني ، بايستي دهيدريشن با نرمال سالين در اولين فرصت ممكن آغاز شود. در بيماران گير افتاده با خروج اولين اندام مايع درماني با سرعت يك ليتر در ساعت آغاز ميشود
بعد از خروج ، سرعت تزريق به 500 سيسي در ساعت نرمال سالين كاهش مييابد و سپس به 1 ليتر در ساعت دكتروز-سالين تبديل ميشود. از تزريق محلولهاي حاوي پتاسيم بخصوص سرمرينگر دوري كنيد
بخش اورژانس مایع درمانی افزودن سديم بيكربنات مانيتول فوروسماید 24 تا 48 ساعت تحت نظر