Download
1 / 90
1.03k likes | 1.33k Views
Frostbite LENG RUPU. Chapter Outline History, Physiology, Pathophysiology, Clinical presentation, Treatment, Sequelae, Prevention. HISTORY.

E N D
Chapter OutlineHistory, Physiology, Pathophysiology, Clinical presentation, Treatment, Sequelae, Prevention
Peripheral cold injuries are almost uniquely seen in humans. Unlike cold-adapted animals, our peripheral tissue temperatures can drop below freezing. The highest homeostatic priority is to maintain the core temperature. This is accomplished through vasoconstriction and shunting, which prevents adequate heat distribution to the extremities. As a result, failure to achieve adequate protection from the environment results in these preventable injuries.
Peripheral cold injuries include both freezing and nonfreezing syndromes. These may occur independently or in conjunction with systemic hypothermia. Frostbite is the most common freezing injury. Trench foot and immersion foot are nonfreezing injuries resulting from exposure to wet cold. Nonfreezing injury following exposure to dry cold is termed chilblains (pernio). one unique aspect of peripheral cold injury is the pathogenesis of the freezing injury cascade.
Most civilian frostbite results from routine exposure without consideration of risk factors. Increased participation in outdoor recreational activities will continue to produce exposure to unanticipated drastic climactic changes. The unsheltered and the homeless are no longer the most likely group at risk.Military history is replete with accounts of the effects of cold injury on combat troops. Trench foot was particularly common among U. S. troops in the Vietnam War.
soldiers would acutely thaw frozen extremities directly over open fires. The subsequent refreeze further increased tissue destruction. Unfortunately, the resultant gangrene was misattributed to this rapid thawing of frostbite and trench foot injuries. Therefore gradual thawing, often including friction massage with snow, remained the standard treatment regimen until the 1950s. In addition to dry radiant heat rewarming and massage, another common rewarming modality was immersion thawing in icy water.
Human cold stress should produce adaptive behavioral reactions in addition to complex endocrinologic and cardiovascular physiologic responses. Peripheral cooling of the blood activates the preoptic anterior hypothalamus. This central thermostat orchestrates temperature regulation. The dynamic process encompasses catecholamine release, thyroid stimulation, shivering thermogenesis, and peripheral vasoconstriction. Consumption of stored fuels is accelerated. The elevated metabolic rate eventually fatigues with a chronic cold insult.
Acral skin structures (fingers, toes, ears, nose) contain a plethora of arteriovenous anastomoses . These facilitate shunting and subsequent drastic reductions in blood flow to these areas. During a cold stress peripheral vasoconstriction limits radiative heat loss. This”life-versus-limb” mechanismreflects the hemeostatic attempt to prevent systemic hypothermia. In contrast to heat exposure, humans do not appear to display significant physiologic adaptation to the cold,
Exposing extremities to cold temperatures down to 15℃ results in maximal peripheral vasoconstriction with minimal blood flow. Continued exposure to progressively colder temperatures down to 10℃ produces the ``hunting response,'' which is termed cold-induced vasodilatation (CIVD).These periods of vasodilatation, recurring in 5-to-10-minute cycles, interrupt vasoconstriction and serve to protect the extremity. Eskimos, as well as Lapps and others of Nordic extraction, are capable of stronger CIVD responses than individuals from tropical regions.
The pathologic phases that occur with local cold injury often overlap and vary with the extent and rapidity of the cold response (see box below). Frostbite occurs when the tissue temperature drops to below 0℃. There are two putative mechanisms of tissue injury: architectural cellular damage from ice-crystal formation and microvascular thrombosis and stasis.
Freezing Injury CascadePrefreeze phase1.Superficial tissue”cooling”2.Increased viscosity of vascular contents3.Microvascular constriction4.Endothelial plasma leakageFreeze-thaw phase1.Extracellular fluid ice-crystal formation*2.Water diapedesis across cell membrane3.Intracellular dehydration and hyperosmolality4.Cell-membrane denaturation/disruption5.Cell shrindage and collapseVascular stasis and progressive ischemia1.Vasospasticity and stasis coagulation2.Arteriovenous shunting3.Vascular endothelial cell damage/prostanoid release4.Interstitial leakage/tissue hypertension5.Necrosis/demarcation/mummification/slough*Extremely rapid cooling produces more initial intracellular than extacellular ice crystallization.
Nerve and muscle tissues are more susceptible to cold injury than connective tissue. For example, nonviable hands and feet can be moved after thawing if the tendons are intact.Edema progresses for 48 to 72 hours after tissue has been thawed. Leukocyte infiltration, thrombosis, and early necrosis become apparent as this edema resolves. The dry gangrene carapace of frostbite is superficial in comparison to arteriosclerotic induced full-thickness gangrene. Final demarcation between viable and nonviable tissue often requires more than 60 to 90 days. Hence the surgical aphorism, ``Frostbite in January, amputate in July”.
Predisposing FactorsPhysiologic PsychologicGenetic Mental statusCore Temperature Fear/panicPrior cold injury Attitude±Acclimatization Peer pressureDehydration FatigueOverexertion Intense concentration on tasksTrauma:multisystem/extremity Hunger; malnutritionDermatologic diseases IntoxicantsPhysical conditioningDiaphoresis/hyperhidrosisEnvironmentalHypoxia Ambient temperature Humidity Cardiovascular Duration of exposureHypotension Wind chill factorAtherosclerosis Altitude±associated conditionsArteritis Orantity of exposed surface areaRaynaud’s syndrome Heat loss: conductive, evaporativeCIVDAnemia MechanicalSickle cell diseaseConstricting/wet clothingDiabetes Tight bootsHypovolemia; shockVapor barrier/alveolite linersVasoconstrictors/vasodilatorsInadequate insulation Immobility/cramped positioning
Symptoms The symptoms of frostbite usually reflect the severity of the exposure. All patients will have some initial sensory deficiency in light touch, pain, or temperature. The most common presenting symptom is numbness, present in over 75% of patients. Anesthesia is produced by intense vasoconstrictive ischemia and neuropraxia. Patients often complain of clumsiness and report a ``chunk of wood'' sensation in the extremity. ``Frostnip'' is a superficial cold insult manifested by transient numbness and tingling that resolves after rewarming. This does not represent true frostbite because there is no tissue destruction.
Chilblains (pernio) is a mild form of dry-cold injury often following repetitive exposure. These ``cold sores'' usually affect facial areas and the dorsum of the hands and feet. Persistent vasospasm and vasculitis result in pruritus, erythema, and mild edema. Plaques, blue nodules, and ulcerations can develop. Trench foot (immersion foot) is produced by prolonged exposure to wet cold at temperatures above freezing. Initially the feet often appear cyanotic, cold, and edematous. There is often numbness and leg cramping. After warming, the skin remains erythematous, dry, and very painful to touch. Vesiculation proceeds to ulceration and liquefaction gangrene in severe cases.
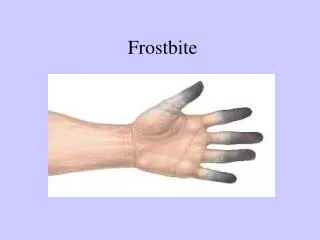
Signs Classically, the initial presentation of frostbite is deceptively benign. Frozen tissues will often appear mottled or violaceouswhite, waxy, or pale yellow. Favorable presenting signs include normal sensation, warmth and color. Soft, pliable subcutaneoustiss.. suggests a superficial injury. A residual violaceous hue after rewarming is ominous. Lack of edema formation may also suggest significant tissue damage. Postthaw edema usually develops in less than 3 hours. In severe cases, frostbitten skin forms an early black, dry eschar until mummification and apparent demarcation.
ClassificationHistorically, frostbite has been classified into degrees of injury similar to burns. Anesthesia and erythema are characteristic of first-degree frostbite. Superficial vesiculation surrounded by edema and erythema is considered second degree. Third-degree frostbite produces deeper hemorrhagic vesicles . Fourth-degree injuries extend into subcuticular osseous and muscle tissues. Classification by degrees is often prognostically incorrect and thus therapeutically misleading. Mills suggests two simple classifications. Superficial or mild frostbite does not entail tissue loss, whereas deep or severe does
Prehospital The ultimate goal of prehospital treatment is preservation of life. Since accidental hypothermia and frostbite often coexist, prevention of further systemic heat loss is the highest priority. Field rewarming of frozen tissue is rarely practical. If possible, remove constricting or wet clothing. Gently insulate and immobilize the affected areas. Friction massage is not efficacious, and will increase tissue loss. Frozen parts should be kept away from dry heat sources in the transport vehicle to prevent a gradual partial thaw.
Emerpency DepartmentPrethaw: obtain pertinent history regarding the ambient temperature, wind velocity, and duration of exposure. Determine the type of apparel and the circumstances surrounding rescue. Document preexistent cardiovascular or neurologic diseases that could affect tissue loss. After stabilizing the core temperature and addressing associated conditions, prepare to initiate rapid thawing. Thaw: Frozen or partially thawed tissue should be rapidly and actively rewarmed by immersion in gently circulating water. Carefully maintain the temperature at 40 to 43℃ by thermometer measurement.
They are invariably hypothermic and at risk for significant fluid and electrolyte fluxes during rewarming. The acute thawing of large amounts of distal musculature extinguishes peripheral vasoconstriction. This results in the sudden return of cold, hyperkalemic, acidotic blood to the central circulation. This ``core temperature after-drop'' is dysrhythmogenic. In the most severe cases, extracorporeal rewarming should be considered to manage these massive metabolic and electrolyte derangements .
Emergency Department Rewarming ProtocolPrethaw•Protectpart•Stabilize core temperature•Address medical/surgical conditions•Hydration•Nofriction massageThaw•Rapid rewarming in 38℃-41℃ circulating water until distal flush (thermometer monitoring)•Requires 10-30 min with active motion of part without friction massage•Parenteral analgesiaPostthaw•Clear vesicles –aspirate (if intact) vs. debride•Hemorrhagic vesicles – aspirate•Apply topical aloe vera (Dermaide) q6h•Ibuprofen 400 mg q12h•Tetanus prophylaxis•Streptococcal prophylaxis for 48-72hr•Elevation
SequelaeNeuropathicPain StricturePhantom Epiphyseal fusionCausalgia Osteoarthritis“Tabes” burning Osteolytic lesionsChronic Necrosis AmputationSensationHypesthesia DermatologicDysesthesia EdemaParesthesia LymphedemaAnesthesia Chronic/recurrent ulcers Epidermoid/squamous carcinomaThermal sensitivity Hair/nail deformitiesHeatCold Miscellaneous Core temperature afterdropAutonomic dysfunction Acute tubular necrosisHyperhidrosis Electrolyte fluxesRaynaud’s Psychic stress GangreneMusculoskeletal SepsisAtrophyCompartment syndromeRhabdomyolysisTenosynovitis
EPIDEMIOLOGY The first report of electrical injury from man-made sources occurred in 1746 after the development of the capacitor. The first recorded death due to electrical current from a man-made source was reported in 1879, when a carpenter in Lyons, France, inadvertently contacted a 250- volt AC dynamo. The first U. S. fatality occured in 1881, when a local inebriate, Samuel W. Smith, passed out on a generator in front of a crowd in Buffalo, New York.
The apparent painlessness of his death impressed the crowd, and electrocution began to be thought of as a ``humane'' mode of execution. In 1890 William Kemmeler became the first man to be put to death in New York State's electric chair. Electrical burns account for 4% to 6.5% of all admissions to burn units
PATHOPHYSIOLOGY The exact pathophysiology of electrical injury is not well understood because of the large number of variables that cannot be measured or controlled when an electrical current passes through tissue. Most of the injury appears to be thermal, and most histologic studies reveal coagulation necrosis consistent with thermal injury. A magnetic field exists wherever an electric current passes, there may be magnetic effects.
Factors Determining Electrical InjuryType of circuitResistance of tissuesAmperageVoltageCurrent pathwayDurationEnvironmental factors
Type of Circuit The type of circuit, alternating current (AC) vs. Direct current (DC), will help to determine the severity of the injury. High-voltage DC tends to cause a single muscle spasm, often throwing the victim from the source. This results in a shorter duration of exposure but increases the likelihood of traumatic blunt injury. It is well-known that contact with a DC source can result in disturbances in cardiac rhythm, depending on the phase of the cardiac cycle affected, a phenomenon that is utilized in the common defibrillator.
AC tends to be three times more dangerous than direct current of the same voltage. The hand is frequently the site of entry as it grasps a tool that comes into contact with an electric source. Because the flexors of the hand and forearm are much stronger than the extensors, contraction of the flexors at the wrist, elbow, and shoulder occur, causing the hand holding onto the current source to pull the source even closer to the body. At currents above the let-go threshold (6 to 9 mA) this can result in the victim's being unable to voluntarily release the current source, prolonging the duration of exposure to the electrical current.
Resistance The Row of electrical energy through a substance is described by Ohm‘s law: R = V/I Resistence(R) of a tissue , electrical energy(I) to thermal energy(P) at any given current as described by Joule's Law: P=I2×R
Duration In general the longer the duration of contact, the greater the degree of tissue destruction.Current Current, expressed in amperes, is a measure of the amount of energy that flows through an object. Voltage Voltage is a measure of potential difference between two points and is determined by the electrical source.
Effects of Amperage Levels in Milli-ampheres(mA)Tingling sensation 1-4Let-go current Children 4 Women 7 Men 9Freezing to circuit 10-20Respiratory arrest from thoracic muscle tetany 20-50Ventricular fibrillation 50-100
Pathway The pathway that a current takes determines the tissues at risk, the type of injury seen, and the degree of conversion of electrical energy to heat. Current passing through the heart or thorax can cause cardiac dysrhythmias and direct myocardial damage. Current passing through the brain can result in respiratory arrest, seizures, and paralysis. Current passing close to the eyes can cause cataracts. It has been suggested that current flowing through the left side of the body may be more dangerous than through the right side or one isolated to an extremity.
As the cross-sectional diameter of the tissue a given current passes through increases the less heat is generated, and less damage occurs as the energy is ``diluted‘’ by the tissue. Because the current is often concentrated at the entrance and exit sites, the greatest degree of damage is often observed there, although deep destruction of the tissues in between may often occur, leading some to describe the surface damage as only ``the tip of the iceberg.
MECHANISMS OF INJURY The mechanisms of electrical injury are listed in the box below. Obviously the victim who becomes part of an electrical circuit, particularly if it is of high voltage, may suffer significant injury. Nonconductive thermal injury can occur by several mechanisms. The most destructive indirect injury occurs when a victim becomes part of an electrical arc. it can cause very deep thermal burns . Sometimes the arc may cause clothing to ignite, resulting in secondary thermal burns. The electrical flash burn. a third mechanism of nonconductive injury, usually results in only superficial partial thickness.
Traumatic injury is frequently seen in patients sustaining electrical injury because they may be thrown clear of the source by intense contraction of their muscles or by falling from a height. The histologic changes seen in muscle injury are coagulation necrosis with shortening of the sarcomere. Vascular damage is greatest in the media, possibly because of the diffusion of heat away from the intima by the flow of blood, but can lead to delayed hemorrhage when the vessel eventually breaks down. Intimal damage may result in either immediate or delayed thrombosis and vascular occlusion
Damage to neural tissue may occur from many mechanisms. It may show an immediate drop in conductivity as it undergoes coagulation necrosis similar to that observed in muscle tissue. In addition, it may suffer indirect damage as its vascular supply or myelin sheath is injured.The brain is frequently injured, focal petechial hemorrhages in the brainstem, widespread chromatolysis, and cerebral edema. Immediate death in electrical injury may be from asystole, ventricullar fibrillation, or respiratory paralysis, depending on the voltage and pathway.
Mechanisms of InjuryDirect contactArcFlashThermalBlunt trauma
Prehospital Considerations When first reaching the scene, paramedic personnel should secure the area so that no other injuries can occur to bystanders or rescuers. It is essential that the power source be turned off Although many approaches to this have been touted, Use of electrical gloves by emergency medical service (EMS) groups has been condemned, A downed high-tension line may jump as it repowers periodically (similar to a water hose that jumps when turned off and on) and may land anywhere in its radius, causing more injuries. Therefore the rescue vehicle should park at least one entire span away from the line.
The victim of an electrical incident should be approached like any other trauma patient because the person may have suffered injury as a result of violent muscle contraction or a fall, in addition to having severe burns that are often more extensive than they initially appear. Attention should be paid to the airway, breathing, and circulation. High-flow oxygen and intubation should be provided if necessary. Cardiac monitoring is essential. If the victim has experienced cardiac arrest, standard advanced life support protocols should be instituted.
Emergency Department Assessment History.Specific injuries: Cardiovascular System. Cardiac arrest, either from asystole or ventricular fibrillation, is a common presenting condition in electrical accidents.Skin. Skin injury are burns. The most common sites of entry for the current include the hands and the skull. The most common areas of exit are the heels. painless, depressed, yellow-grey, punctate areas with central necrosis.
Extremities. Muscle necrosisMassive release of myoglobin from the damaged muscle may lead to myoglobinuric renal failure. Vascular damageDamage to the vessel wall at the time of injury can result in delayed thrombosis and hemorrhage, especially in the small arteries to the muscle. Progressive loss of muscle because of vascular ischemia downstream from damaged vessels may lead to the need for repeated deep debridements.
`kissing burn," occurs at the flexor creases.Nervous System. Loss of consciousness is common and usually transient, Patients may exhibit confusion flat affect, and difficulty with short-term memory and concentration. A seizure may occur after electrical injury . Peripheral nerve damage in extremities sustaining injury is common, and recovery is usually poor.