Download
1 / 57
750 likes | 1.31k Views
RENAL FUNCTION. Study Guide. Module Focus. The kidney plays a major role in the maintenance of fluid and electrolyte balance. elimination of nitrogenous (nitrogen containing ) waste products of protein catabolism (breakdown) Urea or BUN (blood urea nitrogen) Creatinine

E N D
RENAL FUNCTION Study Guide
Module Focus • The kidney plays a major role in the maintenance of • fluid and electrolyte balance. • elimination of nitrogenous (nitrogen containing) waste products of protein catabolism (breakdown) • Urea or BUN (blood urea nitrogen) • Creatinine • The kidneys also synthesize and secrete certain hormones.
Afferent arteriole: the kidney receives 1200 – 1500 ml of blood per minute NEPHRON
First part of nephron “glomus” means ball of yarn Capillary tuft Function: Filters blood Allows smaller subtances that are <70,000 MW to pass from blood to tubular filtrate Filters 125 – 130 ml of plasma per minute “glomerular filtration rate” or GFR Conserves most proteins or protein bound substances such as blood cells which are too large to be filtered Filtrate = “cell-free fluid” GLOMERULUS
Extended end of renal tubule Contains ultrafiltrate of plasma BOWMAN’S CAPSULE
Reabsorbs or returns valuable substances back into blood Returns 75-80% of H2O Returns amino acids & vitamins Ions such as sodium, potassium, chloride, bicarbonate, magnesium & calcium Returns “renal threshold” substances such as glucose as long as the maximum concentration is not exceeded in the plasma (160 – 180 mg/dl) the excess the tubules cannot reabsorb will spill into the urine PROXIMAL TUBULES
PROXIMAL TUBULES • Excreteswaste products into tubular lumen (urine) • Urea (BUN) • Creatinine • Secretes waste products such as hydrogen ions and certain drugs from the blood into the tubular lumen (urine)
LOOP OF HENLE • Concentrates filtrate and adjusts urine osmolality • Descending loop is permeable to water • Ascending loop is impermeable to water
DISTAL TUBULES • Small adjustments are made to achieve electrolyte and acid-base homeostasis • The hormone aldosterone is secreted by the adrenal cortex in response to a decreased blood flow • Aldosterone stimulates the reabsorption of sodium and the loss of potassium sodium levels in blood potassium and hydrogen levels in blood • Reabsorption of more water and bicarbonate also take place • Elimination of ammonia, hydrogen ions and uric acid
COLLECTING DUCTS • Determines final urine osmolality or concentration • Antidiuretic hormone (ADH) is secreted by the posterior pituitary gland in response to an increase in blood osmolality or decrease in blood volume. • ADH stimulates water reabsorption by making the walls permeable to water.
FUNCTIONS OF THE KIDNEY • Water balance maintained by: • Ingestion of water • Excretion & reabsorption of water in renal tubules under the influence of ADH • Electrolyte balance • Sodium, potassium, phosphate, calcium and magnesium • Maitained by tubule reabsorption under influence of aldosterone • Acid-Base balance • Conserve bicarbonate (HCO3-) • Excretes hydrogen ions (H+)
ELIMINATION OF NON-PROTEIN NITROGEN SUBSTANCES • NPN substances = compounds that contain nitrogen, but are not considered proteins • Urea (also known as blood urea nitrogen “BUN”) • Creatinine • Ammonia • Uric acid
SYNTHESIS OF HORMONES • Renin – which is a vasoconstrictor that aids in the regulation of sodium balance and blood pressure • Erythropoietin – which increases hemoglobin production by stimulating RBC production • 1,25-dihydroxycholecalciferol, the active form of Vitamin D, which facilitates calcium absorption from the intestine • Prostaglandins – which affect renal blood flow
Physical properties Chemical analysis pH Protein Glucose Bilirubin blood Microscopic analysis Cells Crystals Casts URINALYSIS
Blood urea nitrogen (BUN) Major waste product of protein breakdown 10 – 20 mg/dl Creatinine Waste product formed in muscle from creatine phosphate Serum = 1.0 mg/dl & urine = 1 – 2 grams per day (constant amount) BUN/Creatinine Ratio Calculation or comparison The ratio of BUN to serum creatinine Normally = 10:1 to 20:1 ratio CHEMISTRY TESTS
CREATININE CLEARANCE • Measurement or calculation of the glomerular filtration rate (GFR) • Considered the most sensitive chemicaltest for assessing kidney function • Collect a 24 hour or timed urine specimen & a blood specimen from the patient • Measure the creatinine in the serum & urine specimen • Calculate the clearance
CLEARANCE CALCULATIONS Urine creatinine mg/dl X Volume of Urine in ml/minute Serum creatinine mg/dl = Creatinine Clearance in ml per minute Reference Ranges = approximately 125 ml/minute
URIC ACID • Not typically used as a renal function test • Because it is a nonprotein nitrogen waste substance, it will be increased in serum if there is any type of renal dysfunction • Useful in the diagnosis of gout – arthritic condition where uric acid deposits in joints & also produces renal calculi
BLOOD UREA NITROGENBUN OR UREA • Composition: O NH2 – C – NH2 To convert BUN to Urea, Multiply the BUN value by 2.14 Since 60 (urea) = 2.14 28 (BUN) Molecular weight N = 14 x 2 = 28 C = 12 O = 16 H = 1 x 4 = 4 Total = 60 gms
SOURCE OF UREA • Major excretory product of proteincatabolism. • Formed in the LIVER from carbon dioxide and ammonia through the urea cycle. CO2 + NH3 = Urea • Excreted by the kidneys • Urea is a small molecule so it is filtered by the glomeruli • Approximately 40 – 70% is reabsorbed by the tubules (the amount reabsorbed is dependent upon the rate of urine flow)
UREASE METHOD 1. The enzyme urease hydrolyzes the urea in the patient specimen to form CO2 & ammonium (NH4) ureaseUREA NH4 + CO2 2. The ammonium is quantitated utilizing the enzyme glutamate dehydrogenase (GLDH) that reduces the coenzyme NADH to NAD with causes a decrease in absorbance that is measured at 340nm. GLDH NH4 + -ketoglutarate + NADH NAD + glutamic acid + H2O
REFERENCE RANGES • BUN is approximately 10 – 20 mg/dl in serum • European labs correctly express BUN as Urea. • To convert, multiply BUN by 2.14 • Example: BUN = 15mg/dl Urea = 15 x 2.14 =
CLINICAL INTERPRETATION INCREASES • Prerenal Factors • Any condition that causes decreased renal perfusion (blood flow) • Congestive heart failure (CHF) • Renal Factors – any renal diseases or disorders • Postrenal Factors -Obstruction such as renal calculi • High protein diet “Dr. Atkin’s diet” will cause mild increases since urea comes from the breakdown of protein. • Cortisol therapy may also cause mild increases.
DECREASES IN BUN • Decreases in BUN are rare & usually insignificant • Pregnancy • Starvation • Severe liver disease - synthesis
CLINICAL INTERPRETATION • BUN is a more sensitive indicator or renal function because it rises earlier and more rapidly than creatinine. • However, it requires approximately 75%loss of nephron function before either BUN or creatinine serum values increase. • BUN is NOT specific because diet (high protein) and cortisol therapy may affect results and cause false increases.
CREATININE SOURCE • Waste product formed in muscle from creatine phosphate • When needed for energy, creatine phosphate and ADP are converted to creatine & ATP • A small portion of creatine phosphate loses its phosphate and creatinine is formed. • Creatinine is excreted in the urine and is NOT usually reabsorbed • The amount of creatinine formed and excreted per day is a function of muscle mass. Typically normal individuals excrete 1 to 2 grams per day of creatinine.
METHODS • Colorimetric: Jaffe Reaction NaOH creatinine + picric acidalkaline picrate (reddish-orange complex) • Noncreatinine chromagens (color-producing substances) such as glucose, ketones and vitamin C may interfere with this reaction • Jaffe KINETIC method modification was designed to monitor the rate of the reaction at selected time intervals to avoid picking up noncreatinine chromagens. (Typically 25 – 60 seconds) • Enzymatic: Creatinine aminohydrolase • A variety of coupled enzymatic methods are available.
REFERENCE RANGES • Serum = 0.8 – 1.4 mg/dl • Urine= 1 – 2 grams per day FYI: • A serum creatinine value of 4mg/dl is equivalent to a reduction of GFR to 15 – 20% of normal. • An 8 mg/dl value = a reduction of GFR to 6 – 10% of normal.
CLINICAL INTERPRETATION INCREASES • Any renal factors • Creatinine is NOT affected by diet • Creatinine is NOT typically reabsorbed by the tubules • Creatinine levels reflect the glomerular filtration rate (GFR)
DECREASES • No medical significance
CLINICAL INTERPRETATION • Creatinine is more specific than BUN since it is not affected by nonrenal factors. • Creatinine is not as sensitive as BUN since serum creatinine levels rise slower than BUN levels. • Remember: Creatinine serum levels are not above normal until ½ to ¾ of kidney function is lost.
BUN-CREATININE RATIO Purpose: • Calculation/comparison that compares the patient’s BUN to their creatinine value • Quality control purposes • Differential diagnosis
EXAMPLE • If a patient’s BUN is approximately 10 – 15mg/dl, their creatinine should be approximately 1.0mg/dl. • This would be equivalent to a 10:1 to 15:1 ratio.
REFERENCE VALUES • 10:1 to 15:1 ratio is considered normal • Normal ratios are usually observed in renal diseases. • Example: If a patient’s BUN is 50 mg/dl, their creatinine would be approximately 5.0 mg/dl.
CLINICAL INTERPRETATION INCREASES: • A 20:1 to 30:1 ratio is often due to prerenal factors • Decreased renal perfusion (blood flow to the kidneys) such as: • Congestive heart failure • Shock, etc. • Causes a >40% reabsorption of urea occurs, but NOT creatinine
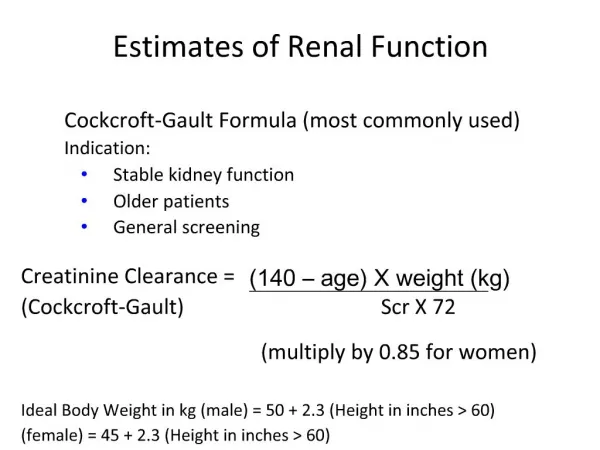
CREATININE CLEARANCE • Estimates the Glomerular Filtration Rate (GFR) by measuring the serum/plasma creatinine level and its rate of excretion into the urine. • Clearance indicates the number of milliliters of plasma from which the kidney can remove all of a given substance in one minute. • The normal GFR is approximately 125 ml/minute.
CLEARANCE REQUIREMENTS • Substance must be filtered through the glomeruli • Essentially no absorbance or secretion must take place in the tubules. • Substance must exist in the same form in the blood and the urine. • Ideally, an endogenous (body-made) substance should be utilized.
PROCEDURE • Collect a timed urine specimen (usually a 24 hour) from the patient. • Record the time period of the collection • Measure and record the total volume of the urine specimen • Collect a blood specimen during the time of the urine collection period. • Measure the urine and serum creatinine in mg/dl. • Calculate the clearance.
Calculate the rate of urine flow or “VOLUME” in ml/minute • Divide the total volume of the urine specimen by the number of MINUTES in the collection period. • Example: • The total volume of a 24hr urine specimen was 1500ml • The number of minutes in a 24hr period would be 24 x 60 = 1440 minutes • Divide 1500ml by 1440 minutes • Volume = 1.04 ml/minute
Clearance Calculations Urine creatinine (mg/dl) X Volume (ml/min) Serum creatinine (mg/dl) Example: A patient’s serum creatinine was 1.0 mg/dl and their urine creatinine was 100 mg/dl. The volume of the 24 hr urine specimen was 1500 ml or 1.04 ml/minute. Clearance = 100 mg/dlX1.04 ml/min= 104 ml/minute 1.0 mg/dl
REFERENCE VALUES • Serum creatinine = 0.8 – 1.4 mg/dl • Urine creatinine = 1- 2 grams per day or 100 mg/100 ml • Total volume = 1000 – 2000 ml/day • Creatinine Clearance • Males: 75 – 140 ml/minute • Females: 70 – 130 ml/minute
CLINICAL INTERPRETATION Remember: You are looking for increased serum values due to the failure of the kidneys to excrete creatinine. This will cause a decrease in urine creatinine as well as a decreased clearance values. DECREASED CLEARANCE VALUES • Acute or chronic damage to the glomeruli • Creatinine clearance is the MOST SENSITIVE chemical indicator of assessing renal function. (more sensitive than serum BUN or serum creatinine)
SOURCES OF ERROR • Error in collection of urine specimen • Calculations • If clearance values are decreased, but the patient’s serum creatinine is normal, check: • Clearance calculations • Urine volume and timing • Incomplete voiding • Incomplete timing • Loss of some urine specimen • Incorrect volume measurement • Urine & serum creatinine values
Increased Clearance Values • No medical significance • Suspect error in collection of urine specimen
Correction of Clearance for Body Surface Area Purpose: Since creatinine is a function of muscle mass, correction is essential if a patient is unusually large or small such as a pediatric patient. Procedure: • Obtain the height & weight of the patient. • Use a nomogram such as the one in your text or study guide to obtain the body surface area of the patient in square meters. • The body surface area of the average patient is assumed to be 1.73 square meters. • Use the following formula to obtain the corrected clearance: Clearance (before correction) X 1.73 M2 Body surface area of patient in M2
URIC ACID Source: • Breakdown of nucleic acids such as RNA & DNA • End product of purine metabolism. • Purines = nitrogen containing constituents of certain coenzymes and nucleic acids. • Derived from endogenous (body made) and exogenous (dietary) nucleoproteins. • Liver, kidneys & shellfish are rich in nucleoproteins.
URIC ACID METABOLISM • Uric acid is synthesized in the liver from the breakdown of nucleic acids. • 90 – 95% is filtered through the glomeruli. • Uric acid is relatively insoluble and will precipitate out of solution if concentration in plasma is > 6.5 mg/dl forming deposits in joints as well as renal calculi (kidney stones). • Mammals other than man are usually capable of oxidizing uric acid to allantoin, which is a more soluble compound.
Methods of Measurement • Phosphotungstic method – outdated • Uricase– enzymatic method is the most widely utilized URICASE Uric acid + O2 + H2O Allantoin + H2O2 + CO2 • Uric acid is oxidized to allantoin and hydrogen peroxide (H2O2) is formed. • A coupled enzymatic reaction, utilizing the enzyme peroxidase, is typically used to quantitate the amount of hydrogen peroxide produced.
Reference Ranges • Males: 3.5 – 7.2 mg/dl • Females: 2.6 – 6.0 mg/dl