Download
1 / 15
150 likes | 154 Views
Lower Limb Claudication Non-Atherosclerotic Pathologies. Dr. Shannon D. Thomas FRACS Vascular, Endovascular and Renal Transplant Surgeon Conjoint Lecturer UNSW Co-Director of Prevocational Education and Training (DPET) Prince of Wales Hospital / Prince of Wales Private Hospital

E N D
Lower Limb ClaudicationNon-Atherosclerotic Pathologies Dr. Shannon D. Thomas FRACS Vascular, Endovascular and Renal Transplant Surgeon Conjoint Lecturer UNSW Co-Director of Prevocational Education and Training (DPET) Prince of Wales Hospital / Prince of Wales Private Hospital Sydney, Australia
Lower Limb Pain Is Common Aetiologies: • Musculoskeletal • Infective • Neurogenic • Atherosclerotic • Venous • Psychological • Compartment Syndrome etc. Non-Atherosclerotic Arterial Disease Uncommon, but affects the young and active
Clinical Features Tend to be <60 years of age Athletic patient Paucity of vascular risk factors Bilateral disease Typical claudication Rest pain and ulcers rare, but possible Difficult to diagnose unless clinically suspicious
Pathologies Popliteal Arterial Entrapment Cystic Adventitial Disease Chronic Compartment Syndrome Bilateral disease Difficult to diagnose unless clinically suspicious
Popliteal Artery EntrapmentClassification • A congenital anomaly • Only becomes clinically apparent when patient starts to exercise • Entrapment of the popliteal artery by the gastrocnemius muscle • Six recognised types
Popliteal Artery EntrapmentDiagnosis • Distal pulses are usually palpable at rest if popliteal artery patent • Pulses may disappear w/ passive dorsiflexion of the foot and active plantar flexion against resistance • (gastrocnemius muscle is tensed across the compressed artery)
Popliteal Artery EntrapmentDiagnosis • Duplex Ultrasound: • with provocation • passive dorsiflexion of the foot • active plantar flexion against resistance • CT Angiogram • with provocation • MRA • identify bands of muscle in popliteal fossa
Popliteal Artery EntrapmentManagement • Release gastrocnemius tendon • Bypass • No role for stents/angioplasty
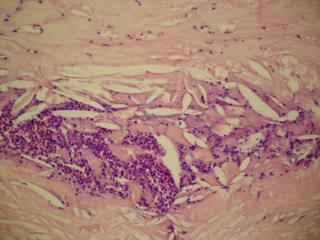
Popliteal Cystic Adventitial Disease • Formation of cysts in the adventitial space of the artery • Leads to stenosis of the lumen • Uncommon, affecting males <60 years of age
Popliteal Cystic Adventitial DiseaseDiagnosis • Stenosis and cysts visible on Duplex Ultrasound • CT/MRI best for diagnosis
Popliteal Cystic Adventitial DiseaseManagement • Covered stenting described but no long term evidence • Cyst excision and patch angioplasty • Popliteal bypass
Chronic Compartment Syndrome • Young athletic patient • Exercise induces excessive compartment pressure leading to nerve and muscle ischaemia • DDx: Shin Splints (Medial Tibial Stress Syndrome)
Chronic Compartment SyndromeDiagnosis • Duplex Scan • MRI: Increased T2-weighted signal in affected post-exercise muscle • Intracompartmental Needle Manometry
Chronic Compartment SyndromeManagement • Physiotherapy • Reduce exercise • Fasciotomy