Download
1 / 175
1.76k likes | 1.99k Views
Introductory Anatomy of Digestive System. NYUNDO Martin, MD, MMed (Surgeon) Lecturer Dpt of Surgery and Dpt of Clinical Anatomy FACMED-NUR.

E N D
Introductory Anatomy of Digestive System NYUNDO Martin, MD, MMed (Surgeon) Lecturer Dpt of Surgery and Dpt of Clinical Anatomy FACMED-NUR
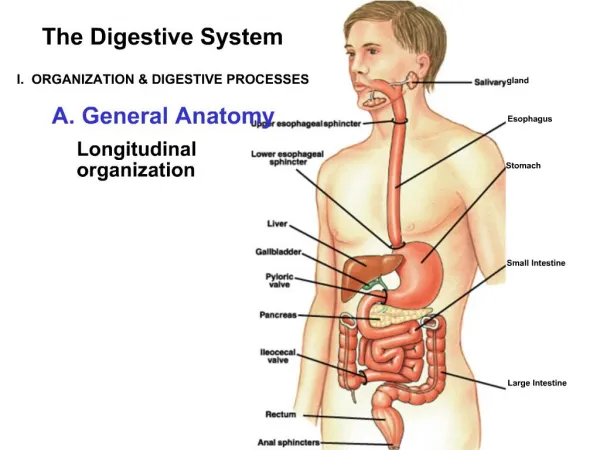
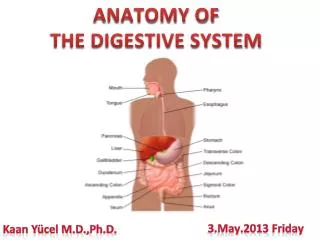
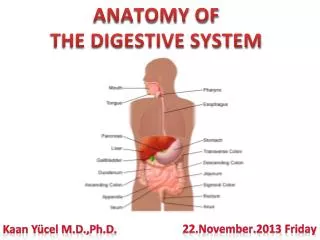
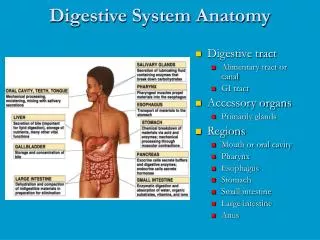
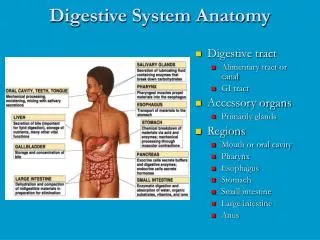
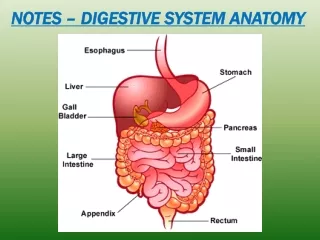
Digestive system is a series of hollow organs joined in a long, twisting tube from the mouth to the anus and other organs that help the body break down and absorb food ►The main organs are: Mouth and pharynx, Oesophagus Stomach, Small and Large intestines,Appendix and Anus ► Accessory organs: Salivary glands, Liver, Gallbladder, Pancreas General considerations
General considerationscont’d • The gastrointestinal tract has a uniform general histology.The GI tract can be divided into 4 concentric layers: • Mucosa is the innermost layer; this layer comes in direct contact with the food (or bolus), and is responsible for absorption and secretion, important processes in digestion. • Submucosa • Muscularis externa (the external muscle layer) • Adventitia or serosa
Accessory organs: • The liver secretes bile into the small intestine via the bile duct, employing the gallbladder as a reservoir. Apart from storing and concentrating bile, the gallbladder has no other specific function. • The pancreas secretes an isosmotic fluid containing bicarbonate, which helps neutralize the acidic chyme, and several enzymes into the small intestine. Both of these secretory organs aid in digestion
General considerationscont’d • Abdomen • The abdomen is the part of the trunk between the thorax and the pelvis • It is a flexible, dynamic container, housing most of the organs of the digestive system and part of the urogenital system. • Containment of the abdominal organs and their contents is provided by: • musculoaponeurotic walls anterolaterally, • diaphragm superiorly, • muscles of the pelvis inferiorly, • lumbar vertebral column in the posterior.
The abdomen encloses and protects its contents while allowing the flexibility between the more rigid thorax and pelvis required by respiration, posture, and locomotion. • Through voluntary or reflexive contraction, its muscular roof, anterolateral walls, and floor can raise internal (intra-abdominal) pressure to aid expulsion from the abdominopelvic cavity or from the adjacent thoracic cavity, expulsion of air from the thoracic cavity (lungs and bronchi) or of fluid (e.g., urine or vomitus), flatus, feces from the abdominopelvic cavity.
General considerationscont’d • Peritoneum and Peritoneal Cavity • The peritoneum is a continuous, glistening and slippery transparent serous membrane. It lines the abdominopelvic cavity and invests the viscera. • The peritoneum consists of two continuous layers: the parietal peritoneum, which lines the internal surface of the abdominopelvic wall, and the visceral peritoneum, which invests viscera such as the stomach and intestines.
The peritoneal cavity is a potential space of capillary thinness between the parietal and visceral layers of peritoneum. • It contains no organs but contains a thin film of peritoneal fluid, which is composed of water, electrolytes, and other substances derived from interstitial fluid in adjacent tissues. • Peritoneal fluid lubricates the peritoneal surfaces, enabling the viscera to move over each other without friction and allowing the movements of digestion.
In addition to lubricating the surfaces of the viscera, the peritoneal fluid contains leukocytes and antibodies that resist infection. • Lymphatic vessels absorb the peritoneal fluid. • The peritoneal cavity is completely closed in males; however, there is a communication pathway in females to the exterior of the body through the uterine tubes, uterine cavity, and vagina. This communication constitutes a potential pathway of infection from the exterior.
General considerationscont’d • Diaphragm • The diaphragm is a double-domed musculotendinous partition separating the thoracic and abdominal cavities. • Its mainly convex superior surface faces the thoracic cavity, and its concave inferior surface faces the abdominal cavity.
The diaphragm is the chief muscle of inspiration. • It descends during inspiration; however, only its central part moves because its periphery, as the fixed origin of the muscle, attaches to the inferior margin of the thoracic cage and the superior lumbar vertebrae. • Orifices: vena caval foramen, esophageal hiatus and aortic hiatus.
Esophagus • First part of the digestive tract, that conveys food from the pharynx to the stomach; it is about 25 cm long and 2 cm of diameter. • Is divided into three anatomical parts: • cervical (superior), thoracic (middle) and abdominal (inferior). • The esophagus: • Follows the curve of the vertebral column as it descends through the neck and mediastinum in the median partition of the thoracic cavity. • Has internal circular and external longitudinal layers of muscle.
In its superior third, the external layer consists of voluntary striated muscle; the inferior third is composed of smooth muscle, and the middle third is made up of both types of muscle. • Passes through the esophageal hiatus in the diaphragm, • Terminates by entering the stomach at the cardial orifice of the stomach
Esophagus cont’d • The esophagus has 2 sphincters: • A sphincter is a narrowing caused by contracted (tightened) muscles. • These muscles remain contracted until the body sends a message for the muscles to relax. When the muscles of the sphincter relax, this then allows things to pass. • One sphincter is at the top of the esophagus. The other is where the esophagus meets the stomach this is known as the gastro-esophageal junction.
The lower sphincter controls the movement of food into the stomach and prevents stomach acid from going up into the esophagus (gastro-esophageal reflux). • The lining of the esophagus is very different to that of the stomach and stomach acid will cause it to become inflamed and sore if reflux does occur.
Stomach • The stomach is the expanded part of the alimentary tract between the esophagus and the small intestine. • It is specialized for the accumulation of ingested food, which it chemically and mechanically prepares for digestion and passage into the duodenum.
RESERVOIR • 2-3L food in adult • 30ml in newborn • SHAPE VARIES • Individual build • Respiration • Contents • Position assumed by individual
Parts of the Stomach: CARDIA the part surrounding the cardial orifice. Orifice at 7th costal cartilage L 2-4 cm from median; at T10 or T11 level FUNDUS - the dilated superior part limited inferiorly by the horizontal plane of the cardial orifice. BODY - the major part of the stomach between the fundus and the pyloric antrum PYLORUS (Pyloric part) From notch - pyloric sphincter At L1-L3 R median plane Stomach cont’d
Stomach cont’d • The stomach has two curvatures: • Lesser curvature: forms the shorter concave border of the stomach • Greater curvature: forms the longer convex border of the stomach • Two surfaces: • Anterior • Posterior
Stomach cont’d Relations • FUNDUS – diaphragm • ANT SURFACE - diaphragm, liver L lobe & ant abd wall • POST SURFACE - omental bursa & retroperitoneal structures (kidney, pancreas, spleen.) • SUPERIOR - lesser omentum & gastric vessels. • INFERIOR - greater omentum & gastro-epiploic vessels.
Stomach cont’d • Principles of blood supply • 2 MAJOR ART SOURCES • Coeliac trunk • Superior mesenteric • VENOUS DRAINAGE • Follow arteries • LYMPHATIC DRAINAGE • Follow arteries
Stomach cont’d • Venous drainage • FOLLOW ARTS • Drain into portal systems • R & L → portal vein • R GASTROEPIPLOIC (G-MENTAL) V → superior mesenteric → may enter portal v direct or join splenic v • L GASTROEPIPLOIC (G-MENTAL) → splenic vein and its tributariess & short gastric vs.
Lymphatic drainage • ALL LYMPH PASSES TO COELIAC GP of pre-aortic nodes • ALL LYMPH VS. ACCOMPANY ARTS along the 2 curves • 4 MAJOR AREAS OF DRAINAGE • LESSER CURV • Largest & drains to L gastric LNs • R PART GREATER CURV • Drains gastroepiploic & pyloric LNs • L PART GREATER CURV • Drains pyl, gastoepip, & pancreticosplenic LNs • LESSER CURVE RELATED TO PYL • Drains to R gastric LNs
Common lymphatics pathway: Drain to coeliac LN → Coeliac trunk →cisterna chyli → Thoracic duct
Nerve supply • PARASYMPATHETIC from ant and post vagal trunks • SYMPATHETIC from coeliac plexus • EFFERENT FIBRES from segments T6-T10 • VAGAL TRUNKS • Ant → lesser curve→ hepatic & duodenal branch • Post → lesser curve from post surface → coeliac → coeliac plexus → post gastric branch
3. SMALL INTESTINES • Extent: stomach to colon • Length: approximately 5m • Parts • Duodenum • Jejunum • Ileum
DUODENUM • The duodenum, the first and shortest (25 cm) part of the small intestine, is also the widest and most fixed part. • The duodenum pursues a C-shaped course around the head of the pancreas. • The duodenum begins at the pylorus on the right side and ends at the duodenojejunal junction on the left side. ( Treitz ligament) • The junction usually takes the form of an acute angle, the duodenojejunal flexure. • Most of the duodenum is fixed by peritoneum to structures on the posterior abdominal wall and is considered partially retroperitoneal.
The duodenum is divisible into four parts: • Superior (first) part: short (approximately 5 cm) and lies anterolateral to the body of the L1 vertebra. • Descending (second) part: longer (7-10 cm) and descends along the right sides of the L1-L3 vertebrae. • Horizontal (third) part: 6-8 cm long and crosses the L3 vertebra. • Ascending (fourth) part: short (5 cm) and begins at the left of the L3 vertebra and rises superiorly as far as the superior border of the L2 vertebra.
Superior or First Part 1 2 4 3 Descending or Second Part Horizontal or Third Part Fourth or Ascending Part
Duodenum blood supply • The arteries arise from the celiac trunk and the superior mesenteric artery. The celiac trunk, via the gastroduodenal artery and its branch, • The veins follow the arteries and drain into the portal vein, some directly and others indirectly, through the superior mesenteric and splenic veins. • The lymphatic vessels of the duodenum follow the arteries.
CLINICALCORRELATES Duodenal ulcer Usual located sup aspect - 1st part When post, penetration may cause bleeding (gastroduodenal art) or erosion into head of pancreas Ant ulcers may perforate into peritoneum (peritonitis).
JEJUNUM & ILEUM Jejunum: 2nd part of the small intestine, begins at the duodenojejunal flexure at the Treitz ligament where the alimentary tract resumes an intraperitoneal course. Wider, thicker-walled than ileum Mucous membrane thrown into circular folds with many longer villi Ileum: third part of the small intestine, ends at the ileocecal junction, the union of the terminal ileum and the cecum . Together, the jejunum and ileum are 6 to 7 m long, the jejunum constituting approximately two fifths and the ileum approximately three fifths of the intraperitoneal section of the small intestine.
Jejunum and ileum • Although no clear line of demarcation between the jejunum and ileum exists, they have distinctive characteristics that are surgically important • The jejunum and ileum can be distinguished by ther color, feel and their complexity of arterial arcades: ♦ Jejum: redder wall, thicker wall(feels full) and simple arcades ♦ Ileum: thinner wall, (feels empty), multiple arcades
The mesentery is a fan-shaped fold of peritoneum that attaches the jejunum and ileum to the posterior abdominal wall • The superior mesenteric artery supplies the jejunum and ileum . • The superior mesenteric vein drains the jejunum and ileum. • Specialized lymphatic vessels in the intestinal villi • Blood vs. arrangement varies jej & ileum
Large Intestine • The large intestine is the site where water is absorbed from the indigestible residues of the liquid chyme, converting it into semisolid stool or feces that is stored temporarily and allowed to accumulate until defecation occurs. • Extent • Ileocaecal junction to anus; about 1.5 m long • Parts: • Caecum & vermiform appendix • Ascending, transverse & descending • Sigmoid • Rectum & anal canal
Large Intestine cont’d • The large intestine can be distinguished from the small intestine by: • Omental appendices: small, fatty, omentum-like projections. • Three teniae coli: • (1) mesocolic, to which the transverse and sigmoid mesocolons attach; • (2) omental, to which the omental appendices attach; and • (3) free (L. libera), to which neither mesocolons nor omental appendices are attached. • Haustra: sacculations of the wall of the colon between the teniae • A much greater caliber (internal diameter). • Mucosa • No villi, numerous mucus cells
Caecum Blind sac invested in peritoneum 8 cm W x 8 cm L, located in RIF Vermiform appendix Attached to posteromedial wall Taenia coli converge on appendix Ileocaecal orifice Opens on medial wall Surrounded by ileocaecal sphincter