Download
1 / 15
150 likes | 254 Views
Carotid Revascularization: Present Patterns of Use, What Will the Future Hold?. John Rumsfeld, M.D., Ph.D., Moderator Live Webcast From: John M. Eisenberg Center for Clinical Decisions and Communications Science Baylor College of Medicine, Houston, Texas. Webcast Agenda. Presentation

E N D
Carotid Revascularization:Present Patterns of Use, What Will the Future Hold? John Rumsfeld, M.D., Ph.D., Moderator Live Webcast From: John M. Eisenberg Center for Clinical Decisions and Communications Science Baylor College of Medicine, Houston, Texas
Webcast Agenda • Presentation • Panel discussion • Question and answer session • Webcast conclusion
Notices • The presentation and panel discussion do not represent the policy of either AHRQ or the U.S. Department of Health and Human Services. • The views expressed are those of the panelists. • No official endorsement by AHRQ or the U.S. Department of Health and Human Services is intended or should be inferred.
Panelists • Lesley H. Curtis, Ph.D., Associate Professor of Medicine, Duke University School of Medicine; Director, Duke DEcIDE Center • Manesh Patel, M.D., Director of Research, Cardiac Catheterization Laboratory at Duke University • Kenneth Rosenfield, M.D., Head of the Section of Vascular Medicine and Intervention, Division of Cardiology, Massachusetts General Hospital
About the Study • Funded by AHRQ’s DEcIDE Network. • Gathers new knowledge and information on specific treatments for the Effective Health Care Program. • Conducted at the DEcIDE Center at Duke University. • Article published in the July 26 issue of Archives of Internal Medicine. • Learn more at: effectivehealthcare.ahrq.gov. DEcIDE = Developing Evidence to Inform Decisions about Effectiveness
Geographic Variation in Carotid Revascularization Among Medicare Beneficiaries, 2003–2006 Presented by: Lesley H. Curtis, Ph.D.
Background • Carotid endarterectomy (CEA) has been the recommended treatment for patients with extracranial carotid artery disease for 20 years. • Percutaneous carotid artery stenting is a therapeutic option of patients at high risk for surgical revascularization. • Results of randomized trials comparing CEA with carotid artery stenting have been mixed.
In October 2004, the Centers for Medicare and Medicaid Services (CMS) issued a national coverage decision supporting the use of carotid stenting for high-risk patients. We analyzed rates of carotid endarterectomy (CEA) and carotid stenting before and after the change in coverage. Background (Continued)
Reviewed all claims for Medicare beneficiaries who underwent CEA or carotid stenting from January 1, 2003 through December 31, 2006. Used HCPCS/CPT codes to identify CEA and carotid stenting and to look for use of carotid imaging studies in the 365 days before the revascularization date. Calculated annual age-adjusted rates of CEA and carotid stenting by hospital referral region (HRR) and calculated rates of carotid imaging prior to revascularization. Summarized all-cause mortality at 30 days and 1 year. Approach
Carotid Revascularization Rates The rate of carotid revascularization was steady at about 3 per 1,000 beneficiaries from 2003 through 2006. Patel MR, et al. Arch Intern Med. 2010;170:1218-1225.
There was a 7- to 9-fold difference between communities (HRRs) with the highest and lowest rates of CEA. 7.2 per 1,000 in Beaumont, TX, as compared to 0.8 per 1,000 in Honolulu, HI. The use of carotid stenting varied by community as well, but there were fewer data available for analysis. 2.7 per 1,000 in St. Joseph, MO, as compared to a national average of 0.4 per 1,000. Geographic Variations Patel MR, et al. Arch Intern Med. 2010;170:1218-1225.
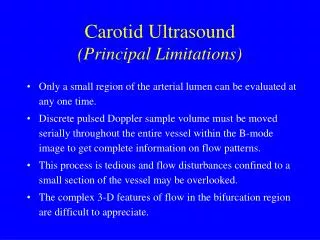
More than 25% of patients in the study received only an ultrasound, while other patients underwent additional imaging tests. Carotid Imaging Prior to Revascularization CEA = carotid endarterectomy; MRA = magnetic resonance angiography Patel MR, et al. Arch Intern Med. 2010;170:1218-1225.
The 30-day all-cause mortality rate for CEA was 1.2% and the 30-day all-cause mortality rate for carotid stenting was 2.3%. Mortality Following Revascularization Patel MR, et al. Arch Intern Med. 2010;170:1218-1225.
Thank you! Join the e-mail list to receive news about the EHC Program!effectivehealthcare.ahrq.gov Close this window to exit the Webcast.