Download

1 / 18
200 likes | 393 Views
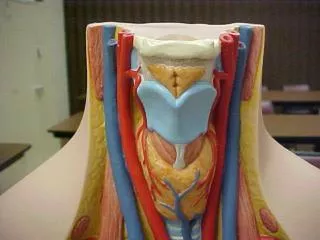
Carotid Artery Palpation. External pressure on carotid artery may slow HR Due to direct stimulation of barorecptor in carotid artery Still appropriate site to measure HR during ex. Cortical Input. Impulses from cerebral cortex pass via small afferent nerves through CVC in medulla

E N D
Carotid Artery Palpation • External pressure on carotid artery may slow HR • Due to direct stimulation of barorecptor in carotid artery • Still appropriate site to measure HR during ex.
Cortical Input • Impulses from cerebral cortex pass via small afferent nerves through CVC in medulla • Allows emotional state to influence CV response • Impulses cause HR to rise rapidly prior to ex. (anticipatory HR)
Probably due to increase in sympathetic discharge and a decrease in vagal tone • Magnitude of increase is greatest in short sprint events and lower in longer events • Represents a 74% increase of HR during a 60 yd sprint • Large portion of HR adjustment to exercise reflects the cortical input that occurs during initial stages of activity • Receptors in joints and muscles (muscle afferents) probably provide a large amount of input to increase HR during initial stages as well
Heart as a pump increase HR increase in SV; limitations Once HR reaches a certain level, strength of contraction decreases, may be due to overuse of substrates in cardiac muscle Period of diastole is so short, cannot fill adequately
with artificial stimulation: peak ability to pump blood is 100-150 bpm • with sympathetic stimulation: increase HR and strength of contraction peak ability: 170-220 bpm
Cardiac Contractility • ΔP/ Δt: rate of change of ventricular pressure with respect to time • way to assess the strength of the contraction of the heart • as ventricular pressure increases at its most rapid rate, the ΔP/ Δt also peaks
usually, rate of rise of ventricular pressure correlates well with strength of ventricular contraction…….. two factors that influence ΔP/ Δt which are not related to cardiac contractility are: 1. Increased input pressure to the left ventricle (EDV, preload) 2. Pressure in the aorta, afterload
Influence of Potassium and Calcium ions Excess potassium in extracellular fluids causes heart to become dilated, flaccid, and slows HR • large quantities can block the cardiac impulse from the atria to the ventricles via AV bundle • elevations of 2-3X normal can weaken heart enough to lead to death
high extracellular potassium concentrations can cause a decrease in the resting membrane potential in cardiac muscle fibers • lower resting membrane potential decrease in AP potential weaker contraction
Excess calcium causes opposite effect • heart goes into spastic contraction • due to direct influence of calcium ions in exciting the cardiac contractile process • deficiency in calcium will cause flaccidity, similar to excess potassium • changes due to calcium are rare, blood levels are tightly controlled
Temperature • increased T will increase HR, sometimes as much as 2X • decreased T will cause decreased HR, as low as few bpm when body temperature is 60-70 F, near death • moderate T increase can enhance the contractile strength of the heart • prolonged elevation in T can cause an exhaustion of the metabolic systems of the heart, causing weakness
Blood Transport arteries carry oxygenated blood (except pulmonary artery) • can withstand high pressures • composed of connective tissue and smooth muscle • from aorta (elastic as well as muscular), through arteries, arterioles, metarterioles, and finally, capillaries • arterioles: smooth muscle; can constrict and dilate dependent on peripheral blood needs • metarterioles are less muscular
capillaries are microscopic blood vessels which contain ~5% of the total blood volume • single layer of endothelial cells, may abut the membranes of surrounding cells • density may be 2-3,000/ mm2 • capillary density is higher in cardiac muscle • precapillary spinchter controls the mouth of the capillary, local control of BF in the capillaries of specific tissues • ~1.5 seconds to pass a blood cell through an average capillary (effective way to exchange)
Blood pressure • surge of blood enters the aorta every time the L ventricle contracts • portion is stored in aorta, arteries and arterioles cannot handle the rapid run off of blood equal to ejection • causes a pressure wave through the arterial system (pulse)
Mean arterial pressure (MAP): average pressure in the arterial system during the cardiac cycle • spend more time in diastole, it is a little less than the average of systole and diastole
Veins • blood flows from capillaries into venules to veins • blood from lower body enters heart via inferior vena cava • blood from the head and shoulders empties into the superior vena cava • when blood enters venules, the impetus for flow is minimal (low pressure)
blood returns via 1. Flap-like valves (one-way) at short intervals in the veins 2. Valves are easily compressed by neighboring muscles couple the one-way valves with the compression, milking action returns blood • 65% of blood volume is in the veins at rest • veins are considered capacitance vessels and reservoirs for blood