Download
1 / 55
550 likes | 665 Views
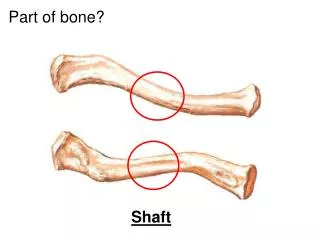
Inherited Diseases of Muscle: Histologic Features. David Lacomis, MD. Classification of Myopathies. Opaque or hyaline fibers. Increase in endomysial connective tissue. Frozen Section from a Patient with Duchenne Muscular Dystrophy. Group of basophilic regenerating fibers.

E N D
InheritedDiseases of Muscle:Histologic Features David Lacomis, MD
Opaque or hyaline fibers Increase in endomysial connective tissue Frozen Section from a Patient withDuchenne Muscular Dystrophy Group of basophilic regenerating fibers
Normal Immunohistochemical Stain for DystrophinSubsarcolemmal staining
Becker Muscular Dystrophy Reduced but present staining split fiber (non-specific chronic change)
Female Carrier of Duchenne Muscular DystrophyA mosaic staining pattern
Female Carrier of Duchenne Muscular DystrophyA mosaic staining pattern
Locations of Affected Proteinsin Muscular Dystrophies Extracellular Matrix Laminin-2 Dystroglycan complex a g a b b sarcoglycans Sarcolemma Lamin A/C (emerin) Caveolin 3 Dysferlin Dystrophin nucleus Actin
Emery-Dreifuss Muscular DystrophyGomori trichrome-stained frozen section Necrotic fiber • Variation in fiber size with many hypertrophic fibers • Increase in endomysial connective tissue • Nonspecific so-called dystrophic changes seen in many of the muscular dystrophies. • Can also be seen in any chronic myopathic disorder. • This disorder is due to loss of the protein emerin.
Myotonic Dystrophy • Chronic changes • Marked excess in internalized nuclei • Variation in fiber sizes • Nuclear clumps (not shown)
H & E, paraffin The excess of internalized nuclei can lead to nuclear chains.
Myotonic DystrophyNADH-reacted section Ring fibers in which myofilaments are organized in different directions
The majority of dystrophies do not have a specific histopathologic appearance. Clinical features are also very important. For example, winging of the scapula is characteristic of FSHD. Fascioscapulohumeral Dystrophy (FSHD)
Variable non-specific changes Range from scattered atrophy to “dystrophic” features. Inflammation can be present. FSH Dystrophy
Basophilic subsarcolemmal structures are sarcoplasmic masses. • Sometimes occur in chronic myopathies such as FSH and myotonic dystrophy.
Variation in muscle fiber size with atrophic angulated fibers Sometimes contain rimmed vacuoles Oculopharyngeal Muscular Dystrophy (OPD)
Higher power view of Gomori trichrome-stained section • Angulated fibers • Fiber containing a large rimmed vacuole
Oculopharyngeal DystrophyGomori trichrome • Ragged red fibers are sometimes seen. • Characteristic of proliferation of abnormal mitochondria.
May be identified by electron microscopy in OPD Intranuclear Filamentous Inclusions
Central areas of absent staining in the dark type I fibers Mitochondria absent Congenital Myopathies: Central Core MyopathyNADH
Congenital Myopathies: Central Core MyopathyNADH • The core consists of disorganized myofibrils and the area is devoid of mitochondria.
Congenital Fiber Type DisproportionH&E • Bimodal size population
Congenital Fiber Type DisproportionATPase pH 4.3 • Smaller fibers are type I • More numerous • Stain lightly • Larger or normal fibers are type II
Nemaline Myopathy • Eosinophilic inclusions present
Nemaline MyopathyGomori trichrome • Eosinophilic inclusions stain darkly
Named for thread-like appearance Inclusions extend from Z-band to Z-band Nemaline MyopathyElectron microscopy
Muscle Biopsy from an Infant • Internalized nuclei predominant • Consistent with centronuclear myopathy • Can be seen in other disorders such as myotonic dystrophy with congenital onset
Muscle Biopsy from an Infant:Centronuclear Myopathy • Central position of the nucleus resembling an embryonic myotube
Metabolic: Inherited – MitochondrialMELAS Syndrome • Ragged red fiber present
MELAS SyndromeSuccinic dehydrogenase reaction • SDH-rich fibers are seen with mitochondrial proliferation
Many COX-negative Fibers • COX-negative fibers are usually seen with mtDNA mutations.
Mitochondrial DisordersElectron Microscopy • Aggregates of mitochondria containing paracrystalline inclusions are frequent. • Non-specific
Mitochondrial DisordersElectron Microscopy Higher power view of paracrystalline inclusion
Oil-red-O stain • Increased lipid storage • Seen in carnitine deficiency states (primary or secondary) • Sometimes as a consequence of certain toxins • Focal increases can be non-specific
Glycogen Storage Myopathies • Some glycogen storage myopathies, such as myophosphorylase deficiency (McArdle’s Disease), cause subsarcolemmal blebs. • PAS-positive due to the presence of glycogen.
McArdles Disease:Phosphorylase Reaction Disease (Absent) Normal Control
McArdle’s DiseaseElectron Microscopy Subsarcolemmal collection of glycogen is shown.
Acid Maltase DeficiencyAcid phosphatase • Due to the intralysosomal activity of this enzyme • Prominent staining with acid phosphatase in vacuoles Vacuolar myopathy noted.
Increased Glycogen • Acid maltase deficiency • Increased glycogen (diffusely and in vacuoles)
Glycogen is digested by diastase in most glycogen storage diseases.