Download
1 / 134
1.35k likes | 1.55k Views
Immunity . Trisha Economidis, MS, ARNP Spring, 2012. WAR DECLARED…. We are at war with our environment Troops are prepared to fight from every sector of the body to keep us safe (and healthy) Regiments on the ready include: Antibodies Immunoglobulins White Blood cells

E N D
Immunity Trisha Economidis, MS, ARNP Spring, 2012
WAR DECLARED….. • We are at war with our environment • Troops are prepared to fight from every sector of the body to keep us safe (and healthy) • Regiments on the ready include: • Antibodies • Immunoglobulins • White Blood cells • Immune Response Teams: Humoral and Cell-Mediated Immunity • And others…….
Immune System Review: Public Enemy Number ONE • Antigen – a protein that stimulates an immune reaction, causing production of antibodies. • Viruses • Bacteria • Fungi • Parasites • Etc…..
Immune System Review • Antibody – a globulin (PRO) produced by B cells as a defense mechanism against foreign materials. Combines in a lock and key style with antigens
First Line of Defense: Primary Defenses • Prevent organisms from entering the body • Skin • Respiratory Tree • Tears/Saliva • Gi Tract – acidic environment, peristalsis • Bile - antimicrobial • GU tract – mucous membranes
Secondary Defenses • Phagocytosis • White blood cells • TO THE RESCUE!
Secondary Defense #2 • Complement Cascade • Set of proteins called complement that trigger release of chemicals that attack the cell membranes of pathogens causing them to rupture
Secondary Defense #3: Inflammation • Begins when histamine and other chemicals are released directly from damaged cells or from basophils in response to complement • Histamine/chemical release Dilation and increased Permeability of blood vessels flow of phagocytes, antimicrobials, O2, & nutrients to area of damage
Secondary Defense #4 • Fever • Increases metabolism • Inhibits pathogen multiplication • Triggers specific immune responses
Tertiary Defenses: Specific Immunity • Body recognizes and destroys pathogens encountered before • Lymphocytes – WBCs that mature to either T cells or B cells
2 Types of Specific Immunity • 1. HumoralImmunity– B (lymphs) cells stimulated to become plasma cells and produce antibodies (immunoglobulins) to the antigens. • Antibodies bind to and destroy antigens.
Specific Immunity No. 2: • Cell-Mediated Immunity: Acts to destroy body cells that have become infected. • T Cells are responsible for cell-mediated immunity: • Cytotoxic (Killer) T cells • Helper T cells • Memory T cells • Suppressor T cells
WBC’s – Name, Rank & Serial Number • Reported in the WBC Differential with a CBC • Basophils 0.5-1% - Release histamine and heparin granules • Eosinophils 1-3% - Destroy helminths, mediate allergic reactions • Monocytes – 3-8% - Phagocytize directly • Lymphocytes (20-35%) – T lymphs – recognize, attack and destroy antigens; B lymphs – produce immunoglobulins to attack and destroy antigens • Neutrophils – 55-70%. First to arrive – Phagocytize! • Bands – Immature neutrophils (normally 3-5% of total WBCs) • Segmented (Segs) – Mature neutrophils –( normally 50-65T of total WBCs)
Shift to the Left?????? • In an acute infection more lymphocytes are produced • A “shift to the left” occurs when there are more bands (immature or baby neutrophils) in circulation than there are segs (mature or grownup neutrophils)
“Shift to the left” • Higher number of bands than segs (usually when bands reach 6%) in circulation called bandemia. • Indicates body is responding to an acute infection, usually bacterial, or to Stress (i.e. women in childbirth)
Immunoglobulins (Ig) – the Special Agents of Humoral Immunity • IgM – Goes after “first time offenders” • IgG – most common one. (AKA: Gamma Globulin) – Active against bacteria and viruses • IgE – primarily responsible for allergic response and parasitic infections • IgA – secreted by mucous membranes around body openings. Provides more protection for points of entry. • IgD – found of surface of B cells. Trap potential pathogens
What are the “weapons” of the Immunoglobulin Agents??? • Phagocytosis • Neutralization • Agglutination • Activation of complement and inflammation
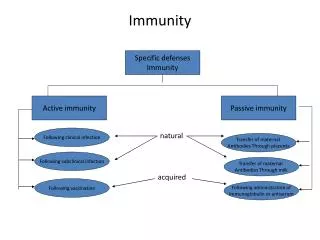
Two Types of Immunity Innate (Native) Adaptive (Acquired) • Present at birth • First line of defense • Non-specific response • Neutrophils first on the site • Cannot be developed or transferred • Body can make it or receive it • Specific response • Results from adaptive response to invasion by an antigen (antibody formation) • Can be passive or active • Can be naturally produced or artificially acquired
Assessment of the Immune system • Chief complaint – subjective data • Review biographic data: age, gender, race, ethnic background, family history • Comprehensive health history • Physical Assessment
Immune System Diagnostics • Allergy testing (will discuss with allergies) • Cd4-T cell counts (Helper T’s) – reflection of immune status (normal: 500-1600 cells/mm3) • Viral Load testing – measures the presence of HIV viral genetic material in the patient’s blood rather than the body’s response to the virus • ELISA/Western Blot • Antibody testing • ANA antinuclear antibody
Immune System Diagnostics • Rheumatoid Factor • Serum Complement • ESR (erythrocyte sedimentation rate) • HLA testing – Human Leukocyte Antigen
Health Promotion and the Immune System – Boosting your Immunity • Diet – Balanced diet • Exercise – Regular, moderate work-outs • Stress relief • Get enough sleep • Use sun exposure protection • Quit smoking or Don’t Start • Avoid Excess alcohol • Immunizations up-to-date
Pharmacologic Management of Immune Disorders • Antibiotics (anti-infectives) • Use: treatment/prophylaxis of bacterial infections • Cautions: Can depress bone marrow; Superinfections • Cephalosporins • Penicillins • Fluoroquinolones • Macrolides • Sulfonamides • Tetracyclines
Pharmacological Interventions • Antivirals – Destroy viruses either directly or by inhibiting the ability to replicate • acyclovir (Zovirax); HSV-1, HSV-2, VZV • osetamivir (Tamiflu), zanamivir (Relenza); Influenza Types A & B
Pharmacological Interventions • Antifungals • Kill or stop growth of fungal infections of skin, mucus membranes, & systemic • Topical • Clotrimazole, ketoconazole, miconazole, nystatin • Systemic • Amphotericin B, fluconazole, ketoconazole
Pharmacological Interventions • Anti-inflammatory • Corticosteroids • Used for anti-inflammatory and immunosuppressive properties • Topical, inhaled, intranasal, opthalmic, IV, PO, IM • Long, intermediate, and short-acting
Pharmacological Interventions • Antihistamines • Relief of symptoms associated with allergies, rhinitis, urticaria • 1st generation-sedating • Chlor-trimeton (chlorpheninamine) • Dramamine (dimenthydrinate) • Benadryl (dephenhydramine) • Atarax, Vistaril (hydroxyzine) • 2nd generation-non-sedating • Allegra (fexofenadine) • Claritin (loratadine) • Zyrtec (cetirizine)
Pharmacological Interventions • Adrenergic sympathomimetic - Epinephrine • Inhibits release of hypersensitivity mediators • Inhibits reaction from mast cells • Produces bronchodilation, vasoconstriction • Epinephrine (Adrenalin) • 0.3mg-0.5 mg subcutaneously or IM (Adults)
Pharmacological Interventions • Immunotherapy • SC injections weekly/biweekly of allergen extracts • Goals of Therapy • Stimulate IgG levels for allergen binding • Decrease IgE levels • ALWAYS EXPECT ADVERSE REACTIONS!!!
Pharmacological Interventions • Biologic Response Modifers (BRMs) • Broad class of drugs that alter the body’s response to diseases such as cancer and autoimmune, inflammatory and infections diseases • Immune Modulators – either enhance or reduce immune responses (some can do both) • Interferons • Monoclonal antibodies • Interleukins • Disease-modifying antirheumatoid arthritis drugs
Pharmacological Interventions • Immunosuppressant Drugs – Decrease or prevent an immune response • cyclosporine (Sandimmune, Neoral, Gengraf) Used to prevent organ rejection in liver, kidney, and heart transplants; treatment of RA and psoriasis. Off-label use in rejection prevention of pancreas, bone marrow, heart/lung transplants. muromonab-CD3 (Orthoclone OKT3) Only one indicated to treat acute organ rejection in kidney, liver and heart transplant
Pharmacological Interventions • Antimalarial (What’s this doing HERE?) • Plaquenil (hydroxychloroquine) – used to decrease joint and muscle pain in early or mild Rheumatoid Arthritis or Lupus (SLE) • Gold Therapy – Rarely used in the U.S. because of toxicities, but may see in patients from other countries. • Antigout – • Acute: colchicine and an NSAID • Chronic: allopurinol (Zyloprim), probenecid (Benemid)
Organ Donation/Transplant:One Boy’s Story http://www.youtube.com/watch?v=yA8671CyM7w7 year old, Nicholas Green
Nursing Management of Clients with Organ Transplants • Transplant success tied to matching tissue antigens, HLA (Human Leukocyte Antigens) • Autograft • Allograft • Xenograft • Histocompatibility – ability of cells and tissues to survive transplantation without immunologic interference by the recipient
Host-versus-Graft Transplant Rejection • Complex process involving both antibody-mediated and cell mediated responses • Hyperacute Rejection – Begins immediately and can’t be stopped once it begins • Acute rejection – occurs 1-3 mo post-transplant. Most common rejection and is treatable. • Chronic rejection – occurs from 4 mos to yrs post-transplant. No cure. Once organ cannot function, another transplant is only course.
Treatment of Transplant rejection Maintenance therapy – Ongoing immune suppressants Ex. cyclosporin, Imuran & a corticosteroid (prednisone) Rescue therapy – treats acute rejection. Ex: ALG , murononab-CD3. Most effective during first course of treatment
What is an allergy? • Allergy is an exaggerated immune response to an antigen (foreign or allergen) to which the patient has been previously exposed. • Also called hypersensitivity
Allergy Terminology • Allergen – an antigen that causes an allergic sensitization • Mast cell – a tissue cell that contains granules filled with chemical mediators such as histamine and heparin. Play a major role in allergies as well as immune system function. • Atopic – relating to a hereditary predisposition toward developing certain allergic reactions
Why does an allergic reaction occur? • 1. First time exposure to an allergen, our body responds by making “antigen-specific” IgE • 2. The antigen-specific IgE binds to the surface of mast cells and basophils (both have granules containing chemical mediators including histamine that will be released when stimulated) • 3. Once the IgE is formed, we are sensitized to that allergen
Hypersensitivity (allergic) Reactions • Type I reaction – occurs when the already sensitized person (see previous slide) is re-exposed to the allergen (IgE mediated) • Histamine and other chemicals are released from the cells • Inflammatory response occurs from other proteins released from the cells that draw more WBC’s to the area
Anaphylaxis – Serious Type I Reaction • Immediate life-threatening systemic reaction • Can occur in seconds to minutes • Not common • Life-threatening and can be fatal • What can cause it: allergy shots, insect bites/stings, foods (peanuts, eggs, shellfish, etc.) medications, blood products, contrast media, exercise, skin testing.
Anaphylaxis – What does it look like? • Respiratory – bronchospasm, laryngeal edema, wheezing, cough • Cardiovascular – hypotension, tachycardia, palpitations, syncope • Skin – urticaria, angioedema, pruitus, erythema • GI – N/V/D/, abdominal pain
Emergency Care • Recognize symptoms • A, B, Cs • Administer drugs -Epinephrine 1:1000 0.3-0.5 mL SQ or Epi-pen 0.3 mL IM (adults), 0.15 mL IM (children) -Oxygen -Antihistamines -Bronchodilators
History of Anaphylaxis? • Obtain Medical Alert Bracelet • Carry Epi-pen
Did I inherit my allergies? • Yes, and no…. • The tendency to produce IgE to certain antigen exposure is based on genetic inheritance. • Allergic tendencies are inherited (atopy); specific allergies are NOT inherited
Other Hypersensitivity Reactions • Type II: Cytotoxic – involve IgG. Body makes antibodies that attack self cells resulting in death of the cell. • Ex. Hemolytic anemias, hemolytic transfusion reactions (person gets wrong blood type in a transfusion)
Hypersensitivity Reactions, cont. • Type III: Immune Complex Reactions – too many circulating antigens form large antigen-antibody complexes that lodge in small blood vessel walls; triggering inflammation and tissue damage. • Type IV: Delayed Hypersensitivity Reactions – Sensitized T cells react to antigens by triggering macrophages to destroy the antigen. • Type V: Stimulatory Reactions - autoantibodies constantly stimulate reaction from normal cells resulting in a “turned on” state continuously
Allergy Testing • Method-Apply to arms or back • Cutaneous scratch or prick • Intradermal (the most accurate) • **Patch (for contact dermatitis) • Response • Produces localized response (wheal & flare) • Diagnostic for allergies to specific antigen • Positive reaction within minutes • Lasts 8-12 hours