Download
1 / 1
10 likes | 207 Views
NPS were collected at UTMB from thirty eight infants and children younger than 24 months from December 2011 to March 2013. The children were recruited from the pediatric outpatient clinics, UTMB Emergency Department, inpatient floor, and pediatric intensive care unit.

E N D
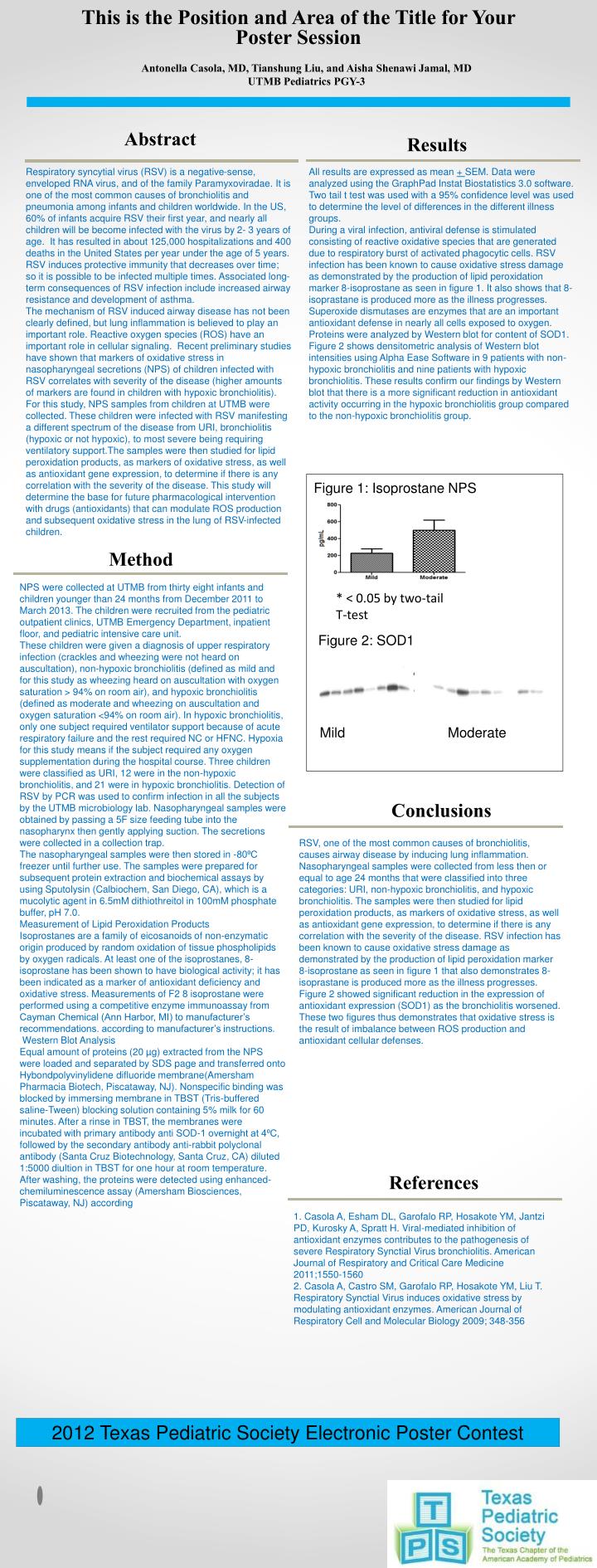
NPS were collected at UTMB from thirty eight infants and children younger than 24 months from December 2011 to March 2013. The children were recruited from the pediatric outpatient clinics, UTMB Emergency Department, inpatient floor, and pediatric intensive care unit. These children were given a diagnosis of upper respiratory infection (crackles and wheezing were not heard on auscultation), non-hypoxic bronchiolitis (defined as mild and for this study as wheezing heard on auscultation with oxygen saturation > 94% on room air), and hypoxic bronchiolitis (defined as moderate and wheezing on auscultation and oxygen saturation <94% on room air). In hypoxic bronchiolitis, only one subject required ventilator support because of acute respiratory failure and the rest required NC or HFNC. Hypoxia for this study means if the subject required any oxygen supplementation during the hospital course. Three children were classified as URI, 12 were in the non-hypoxic bronchiolitis, and 21 were in hypoxic bronchiolitis. Detection of RSV by PCR was used to confirm infection in all the subjects by the UTMB microbiology lab. Nasopharyngeal samples were obtained by passing a 5F size feeding tube into the nasopharynx then gently applying suction. The secretions were collected in a collection trap. The nasopharyngeal samples were then stored in -80⁰C freezer until further use. The samples were prepared for subsequent protein extraction and biochemical assays by using Sputolysin (Calbiochem, San Diego, CA), which is a mucolytic agent in 6.5mM dithiothreitol in 100mM phosphate buffer, pH 7.0. Measurement of Lipid Peroxidation Products Isoprostanes are a family of eicosanoids of non-enzymatic origin produced by random oxidation of tissue phospholipids by oxygen radicals. At least one of the isoprostanes, 8-isoprostane has been shown to have biological activity; it has been indicated as a marker of antioxidant deficiency and oxidative stress. Measurements of F2 8 isoprostane were performed using a competitive enzyme immunoassay from Cayman Chemical (Ann Harbor, MI) to manufacturer’s recommendations. according to manufacturer’s instructions. Western Blot Analysis Equal amount of proteins (20 µg) extracted from the NPS were loaded and separated by SDS page and transferred onto Hybondpolyvinylidene difluoride membrane(Amersham Pharmacia Biotech, Piscataway, NJ). Nonspecific binding was blocked by immersing membrane in TBST (Tris-buffered saline-Tween) blocking solution containing 5% milk for 60 minutes. After a rinse in TBST, the membranes were incubated with primary antibody anti SOD-1 overnight at 4⁰C, followed by the secondary antibody anti-rabbit polyclonal antibody (Santa Cruz Biotechnology, Santa Cruz, CA) diluted 1:5000 diultion in TBST for one hour at room temperature. After washing, the proteins were detected using enhanced-chemiluminescence assay (Amersham Biosciences, Piscataway, NJ) according This is the Position and Area of the Title for Your Poster Session Antonella Casola, MD, Tianshung Liu, and Aisha Shenawi Jamal, MD UTMB Pediatrics PGY-3 Abstract Results Respiratory syncytial virus (RSV) is a negative-sense, enveloped RNA virus, and of the family Paramyxoviradae. It is one of the most common causes of bronchiolitis and pneumonia among infants and children worldwide. In the US, 60% of infants acquire RSV their first year, and nearly all children will be become infected with the virus by 2- 3 years of age. It has resulted in about 125,000 hospitalizations and 400 deaths in the United States per year under the age of 5 years. RSV induces protective immunity that decreases over time; so it is possible to be infected multiple times. Associated long-term consequences of RSV infection include increased airway resistance and development of asthma. The mechanism of RSV induced airway disease has not been clearly defined, but lung inflammation is believed to play an important role. Reactive oxygen species (ROS) have an important role in cellular signaling. Recent preliminary studies have shown that markers of oxidative stress in nasopharyngeal secretions (NPS) of children infected with RSV correlates with severity of the disease (higher amounts of markers are found in children with hypoxic bronchiolitis). For this study, NPS samples from children at UTMB were collected. These children were infected with RSV manifesting a different spectrum of the disease from URI, bronchiolitis (hypoxic or not hypoxic), to most severe being requiring ventilatory support.The samples were then studied for lipid peroxidation products, as markers of oxidative stress, as well as antioxidant gene expression, to determine if there is any correlation with the severity of the disease. This study will determine the base for future pharmacological intervention with drugs (antioxidants) that can modulate ROS production and subsequent oxidative stress in the lung of RSV-infected children. All results are expressed as mean + SEM. Data were analyzed using the GraphPad Instat Biostatistics 3.0 software. Two tail t test was used with a 95% confidence level was used to determine the level of differences in the different illness groups. During a viral infection, antiviral defense is stimulated consisting of reactive oxidative species that are generated due to respiratory burst of activated phagocytic cells. RSV infection has been known to cause oxidative stress damage as demonstrated by the production of lipid peroxidation marker 8-isoprostane as seen in figure 1. It also shows that 8-isoprastane is produced more as the illness progresses. Superoxide dismutases are enzymes that are an important antioxidant defense in nearly all cells exposed to oxygen. Proteins were analyzed by Western blot for content of SOD1. Figure 2 shows densitometric analysis of Western blot intensities using Alpha Ease Software in 9 patients with non-hypoxic bronchiolitis and nine patients with hypoxic bronchiolitis. These results confirm our findings by Western blot that there is a more significant reduction in antioxidant activity occurring in the hypoxic bronchiolitis group compared to the non-hypoxic bronchiolitis group. Figure 1: Isoprostane NPS Method * < 0.05 by two-tail T-test Figure 2: SOD1 Mild Moderate Conclusions RSV, one of the most common causes of bronchiolitis, causes airway disease by inducing lung inflammation. Nasopharyngeal samples were collected from less then or equal to age 24 months that were classified into three categories: URI, non-hypoxic bronchiolitis, and hypoxic bronchiolitis. The samples were then studied for lipid peroxidation products, as markers of oxidative stress, as well as antioxidant gene expression, to determine if there is any correlation with the severity of the disease. RSV infection has been known to cause oxidative stress damage as demonstrated by the production of lipid peroxidation marker 8-isoprostane as seen in figure 1 that also demonstrates 8-isoprastane is produced more as the illness progresses. Figure 2 showed significant reduction in the expression of antioxidant expression (SOD1) as the bronchiolitis worsened. These two figures thus demonstrates that oxidative stress is the result of imbalance between ROS production and antioxidant cellular defenses. References 1. Casola A, Esham DL, Garofalo RP, Hosakote YM, Jantzi PD, Kurosky A, Spratt H. Viral-mediated inhibition of antioxidant enzymes contributes to the pathogenesis of severe Respiratory Synctial Virus bronchiolitis. American Journal of Respiratory and Critical Care Medicine 2011;1550-1560 2. Casola A, Castro SM, Garofalo RP, Hosakote YM, Liu T. Respiratory Synctial Virus induces oxidative stress by modulating antioxidant enzymes. American Journal of Respiratory Cell and Molecular Biology 2009; 348-356 * < 0.05 by two-tail T-test Figure 2: SOD 1 2012 Texas Pediatric Society Electronic Poster Contest



















