Download
1 / 1
10 likes | 146 Views
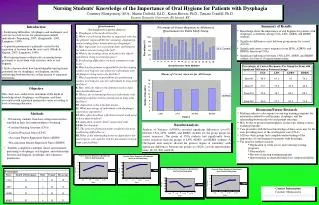
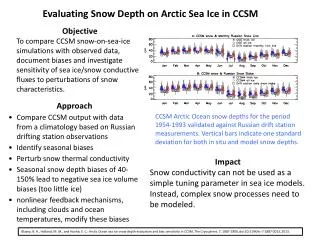
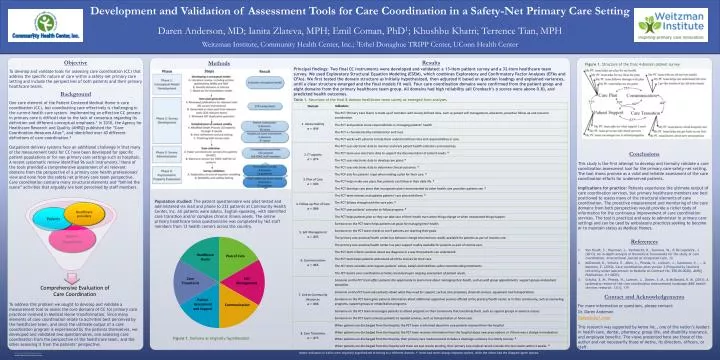
Figure 1. Structure of the final 4-domain patient survey. Table 1. Structure of the final 8-domain healthcare team survey as emerged from analyses. For more information or questions, please contact: Dr. Daren Anderson Daren@chc1.com

E N D
Figure 1. Structure of the final 4-domain patient survey Table 1. Structure of the final 8-domain healthcare team survey as emerged from analyses For more information or questions, please contact: Dr. Daren Anderson Daren@chc1.com This research was supported by Aetna Inc., one of the nation’s leaders in health care, dental, pharmacy, group life, and disability insurance, and employee benefits. The views presented here are those of the author and not necessarily those of Aetna, its directors, officers, or staff. Methods Background Results Conclusions This study is the first attempt to develop and formally validate a care coordination assessment tool for the primary care safety-net setting. The tool shows promise as a valid and reliable assessment of the care coordination efforts for underserved patients. Implications for practice: Patients experience the ultimate output of care coordination services, but primary healthcare members are best positioned to assess many of the structural elements of care coordination. The proactive measurement and monitoring of the core domains from both perspectives would provide a richer body of information for the continuous improvement of care coordination services. The tool is practical and easy to administer in primary care settings and can be used by ambulatory practices seeking to become or to maintain status as Medical Homes. References Van Houdt, S., Heyrman, J., Vanhaecht, K., Sermeus, W., & De Lepeleire, J. (2013). An in-depth analysis of theoretical frameworks for the study of care coordination. International journal of integrated care, 13. McDonald, K., Schultz, E., Albin, L., Pineda, N., Lonhart, J., Sundaram, V., ... & Malcolm, E. (2010). Care coordination atlas version 3 (Prepared by Stanford University under subcontract to Battelle on Contract No. 290-04-0020). AHRQ Publication, (11-0023). Schultz, E. M., Pineda, N., Lonhart, J., Davies, S. M., & McDonald, K. M. (2013). A systematic review of the care coordination measurement landscape.BMC health services research, 13(1), 119. Contact and Acknowledgements Population studied: The patient questionnaire was pilot tested and administered via mail and phone to 232 patients at Community Health Center, Inc. All patients were adults, English-speaking, with identified care transition and/or complex chronic illness needs. The online primary healthcare team questionnaire was completed by 162 staff members from 12 health centers across the country. Principal findings: Two final CC instruments were developed and validated: a 13-item patient survey and a 32-item healthcare team survey. We used Exploratory Structural Equation Modeling (ESEM), which combines Exploratory and Confirmatory Factor Analyses (EFAs and CFAs). We first tested the domain structure as initially hypothesized, then adjusted it based on question loadings and explained variances, until a clear structure emerged and the final models fit well. Four care coordination domains were confirmed from the patient group and eight domains from the primary healthcare team group. All domains had high reliability (all Cronbach’s α scores were above 0.8), and predicted health outcomes. To develop and validate tools for assessing care coordination (CC) that address the specific nature of care within a safety-net primary care setting and include the perspectives of both patients and their primary healthcare teams. Daren Anderson, MD; Ianita Zlateva, MPH; Emil Coman, PhD1; Khushbu Khatri; Terrence Tian, MPH Weitzman Institute, Community Health Center, Inc.; 1Ethel Donaghue TRIPP Center, UConn Health Center Development and Validation of Assessment Tools for Care Coordination in a Safety-Net Primary Care Setting One core element of the Patient Centered Medical Home is care coordination (CC), but coordinating care effectively is challenging in the current health care system. Implementing an effective CC process in primary care is difficult due to the lack of consensus regarding its definition and different conceptual emphases.1In 2010, the Agency for Healthcare Research and Quality (AHRQ) published the “Care Coordination Measures Atlas”, and identified over 40 different definitions of care coordination.2 Outpatient delivery systems face an additional challenge in that many of the measurement tools for CC have been developed for specific patient populations or for non-primary care settings such as hospitals. A recent systematic review identified 96 such instruments.3 None of the tools provided a comprehensive assessment of all relevant domains from the perspective of a primary care health professionals’ view and none from the safety net primary care team perspective. Care coordination contains many structural elements and “behind the scene” activities that arguably are best perceived by staff members. To address this problem we sought to develop and validate a measurement tool to assess the core domains of CC for primary care practices involved in Medical Home transformation. Since many elements of care coordination relate to activities best perceived by the healthcare team, and since the ultimate output of a care coordination program is experienced by the patients themselves, we developed and validated two questionnaires, one assessing care coordination from the perspective of the healthcare team, and the other assessing it from the patients’ perspective. Objective Figure 1. Domains as originally hypothesized Notes: Indicators in italics were originally hypothesized to belong to a different domain; N: items had never/always response options, while the others had the disagree/agree options.