Download
1 / 33
330 likes | 450 Views
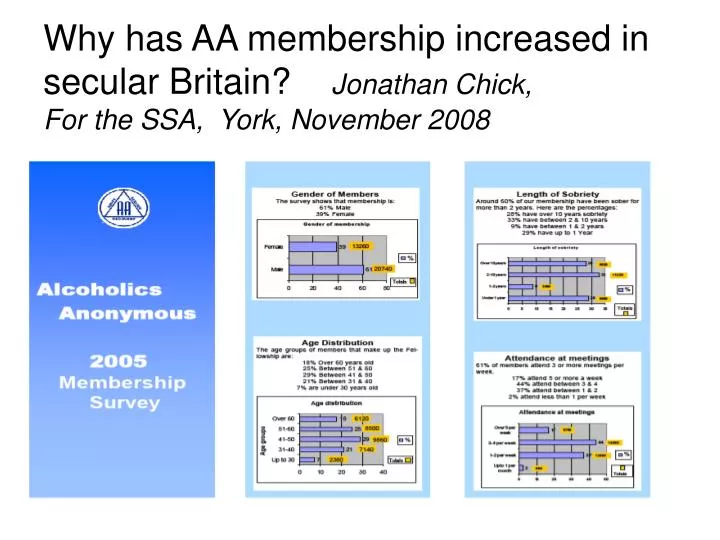
Why has AA membership increased in secular Britain? Jonathan Chick, For the SSA, York, November 2008. Alcoholics Anonymous in the UK. Survey 1986 : 2176 groups, ?18,000 members Survey 2005 : 3630 groups, about 34,000 members Estimate 2008: 4000 groups, about 40,000 members.

E N D
Why has AA membership increased in secular Britain? Jonathan Chick, For the SSA, York, November 2008
Alcoholics Anonymous in the UK Survey 1986 : 2176 groups, ?18,000 members Survey 2005 : 3630 groups, about 34,000 members Estimate 2008: 4000 groups, about 40,000 members.
Clinical Effectiveness derived from meta-analysis: applied to 1000 cases Scottish Health Technology Assessment
You can’t learn to navigate in a ship that’s sinking • Hence Antabuse, Campral, and perhaps other medications, can help in early recovery
Evidence for AA? • No true randomised controlled study • Many follow-up studies show that stable recovery is associated with regular attendance at AA / NA e.g. London, UK Gossop et al (2007) 5-year follow-up after residential treatment for drug dependence ADDICTION, 103, 119-125 Gossop et al (2003)6-month follow-up after in-patient treatment for alcoholism ALCOHOL & ALCOHOLISM 38:421-6.
Social Recovery Model: An 8-Year Investigation of Adolescent 12-Step Group Involvement Following Inpatient Treatment.Kelly JF, et al Alcohol Clin Exp Res. 2008 [Epub ahead of print] • Adolescent inpatients (n = 160; mean age = 16, 40% female). • Conclusions: Even though many youth discontinue AA/NA over time, attendees appear to benefit, and more severely substance-involved youth attend most.
Enhanced friendship networks and active coping mediate the effect of self-help groups on substance abuse • 2,337 male veterans treated for substance abuse. • The majority of participants became involved in self-help groups after inpatient treatment • group involvement predicted reduced substance use at 1-year follow-up. • enhanced friendship networks and increased active coping responses appeared to mediate these effects Humphreys et al . 1999 Ann Behav Med21:54-60
4-year outcome of community residential treatment for patients with substance use disorders.Laffaye et al. Addiction. 2008 103:671-80. • 2324 male patients • At 1-year follow-up, being employed and greater use of AA-related coping predicted outcome significantly. • AA-related coping at 1 year mediated the relationship partially between belief in AA philosophy at treatment entry and 4-year outcome.
Is attendance at Alcoholics Anonymous meetings after inpatient treatment related to improved outcomes? A 6-month follow-up study. • Gossop M, Harris J, Best D, Man LH, Manning V, Marshall J, Strang J. • National Addiction Centre, Maudsley Hospital/Institute of Psychiatry, 4 Windsor Walk, London SE5 8RF, UK. m.gossop@iop.kcl.ac.uk • AIMS: This study investigates the relationship between attendance at Alcoholics Anonymous (AA) meetings prior to, during, and after leaving treatment, and changes in clinical outcome following inpatient alcohol treatment. METHODS: A longitudinal design was used in which participants were interviewed at admission (within 5 days of entry), and 6 months following departure. The sample comprised 150 patients in an inpatient alcohol treatment programme who met ICD-10 criteria for alcohol dependence. The full sample was interviewed at admission to treatment. Six months after departure from treatment, 120 (80%) were re-interviewed. RESULTS: Significant improvements in drinking behaviours (frequency, quantity and reported problems), psychological problems and quality of life were reported. Frequent AA attenders had superior drinking outcomes to non-AA attenders and infrequent attenders. Those who attended AA on a weekly or more frequent basis after treatment reported greater reductions in alcohol consumption and more abstinent days. This relationship was sustained after controlling for potential confounding variables. Frequent AA attendance related only to improved drinking outcomes. Despite the improved outcomes, many of the sample had alcohol and psychiatric problems at follow-up. CONCLUSIONS: The importance of aftercare has long been acknowledged. Despite this, adequate aftercare services are often lacking. The findings support the role of Alcoholics Anonymous as a useful aftercare resource.
Project MATCH Research groupAddiction 1997;92:1671-98 Out-patients N=952 Aftercare following in-patient stay N=774 Random allocation to: 12 sessions cognitive behavioral therapy-CBT or 12 sessions of twelve-step facilitation-TSF or 4 sessions of motivational enhancement therapy - MET
PROJECT MATCH: 1 year outcome • No differences on number of days drinking or amount drunk per day • Time to First Drink, and Time to 3 Successive Heavy Drinking Days, better in TSF than CBT or MET • Highly dependent did best in TSF (low dependence better in CBT) At 3 years, still slight advantage on some measures to TSF (Only 40% of TSF patients regularly attended AA)
Longabough R, et al Network support for drinking: Alcoholics Anonymous and long-term matching effects. Addiction 1998; 93:1313-1334
Scottish cost-effectiveness studyHealth Technology Board of Scotland Slattery et alPrevention of Relapse in Alcohol Dependencewww.docs.scottishmedicines.org/docs/pdf/Alcohol%20Report.pdf‘Patientsshould be encouraged to attend AA, particularly those who live or work in environments where there is a lot of drinking and little support for abstinence’ Cost - Nil Cost-effectiveness = ∞
Controlled trial of intensive referral to 12 step self help groups: One year outcomes Timko and DeBenedetti, Drug Alc Depend 2007; 90:270-9 • N=345 METHODS: In this randomized controlled trial, individuals with substance use disorders (SUDs) entering a new outpatient treatment episode (N=345; 96% had previous SUD treatment) were randomly assigned to a standard referral or an intensive referral-to-self-help condition and provided self-reports of 12-step group attendance and involvement and substance use at baseline and at six-month and one-year follow-ups (93%). In. Intensive referral had the key elements of counselors linking patients to 12-step volunteers and using 12-step journals to check on meeting attendance. RESULTS: Compared with patients who received standard referral, patients who received intensive referral were more likely to attend and be involved with 12-step groups during both the first and second six-month follow-up periods, and improved more on alcohol and drug use outcomes over the year. Specifically, during both follow-up periods, patients in intensive referral were more likely to attend at least one meeting per week (70% versus 61%, p=.049) and had higher SHG involvement (mean=4.9 versus 3.7, p=.021) and abstinence rates (51% versus 41%, p=.048). Twelve-step involvement mediated the association between referral condition and alcohol and drug outcomes, and was associated with better outcomes above and beyond group attendance. CONCLUSIONS: The intensive referral intervention was associated with improved 12-step group attendance and involvement and substance use outcomes. To most benefit patients, SUD treatment providers should focus 12-step referral procedures on encouraging broad 12-step group involvement, such as reading 12-step literature, doing service at meetings, and gaining self-identity as a SHG member.
Interpersonal learning Catharsis Group cohesiveness Self-understanding Development of socialising techniques Existential factors Universality Instillation of hope Altruism Corrective family re-enactment Guidance Identification/imitative behaviour Yalom's curative factors in group therapy (1970)
Psychological theories of addictions Social control theory: weak bonds/ poor monitoring/deviant values Social learning theory expectancies/peer pressure Behavioural economics (choice) theory –reward competition. Stress and coping theory: conflict,abuse / impulsivity/ avoidance Active ingredients of Self Help Groups New norms: new friends; sponsor; observe New role models Engagement in rewarding activities sharing/making tea!/ helping others Self efficacy and coping skills Active ingredients of substance use-focused self-help groupsMoos (2008) Addiction,103,387-396
What patients initially dislike about AA • Catch-phrases\clichés - the trite pinned up notices • ‘God as we understood him’ • ‘Higher Power’
What patients initially like about AA • The humour • The Catch phrases – you hear them so often, they pop into your mind when you’re vulnerable: ‘One’s too many, 10’s not enough’ • “You feel calm when you leave a meeting, (after the despair you felt when drinking)” • ‘Everyone is so friendly’
Spirituality: Whatever is that? ‘It is not necessary to hold formal religious beliefs, or engage in religious practices, or belong to an established faith tradition, to experience the spiritual dimension’ Royal College of Psychiatrists
Spirituality is identified with experiencing a deep-seated sense of meaning and purpose in life, together with a sense of belonging. It is about acceptance, integration and wholeness.
Spirituality = ‘Higher Power’ • “linking the deeply personal with the universal”, • inclusive and unifying. • leads to the recognition that to harm another is to harm oneself, and equally that helping others is to help oneself. It applies to everyone, including those who do not believe in God or a ‘higher being’.
Do you experience a feeling of belonging and being valued, a sense of safety, respect and dignity? • Is there openness of communication both ways between you and other people?
Fostering an awareness that serves to identify and promote values such as: creativity, patience, perseverance, honesty, humility kindness, compassion, equanimity, hope and joy
Spiritual skills include • being self-reflective and honest; • being able to remain focused in the present, remaining alert, unhurried and attentive; • being able to rest, relax and create a still, peaceful state of mind; • developing greater empathy for others; • finding courage to witness and endure distress while sustaining an attitude of hope; • developing improved discernment, for example about when to speak or act and when to remain silent; • learning how to give without feeling drained; • being able to grieve and let go. Sounds like desired outcomes of good psychotherapy? (Many studies show lack of emotional/affective understanding in alcoholics, not due to family history but to the drinking eg Monnot et al 2001, Alcohol Clin Exp Res 25:362-9.) Royal College of Psychiatrists
The alcoholic believes his drinking is the result of poor will-power • and he can only stop drinking by an act of will Nineteenth-century ideas about the primacy of the individual, taken up by psychoanalysis, continue to dominate Western culture. • e.g. Mrs Thatcher's famous remark "I don't believe in society. There is no such thing, only individual people, and there are families" (Women's Own, 31 October 1987) • As long as he sees his drinking as a failing rather than a biological condition+socialisation, he will seek a solution within himself. • His beliefs are self-fulfilling prophecies
Handing over to a Higher Power • Ceasing believing that you are in control of your addiction • Accepting the group’s strength • Being more humble • Relinquish control, follow others’ advice • Acknowledge your weakness, allows you to find new strength -your higher power-whatever that means for you • Accepting what cannot be changed (and having the courage to change what can be changed)
Do not hand over to a psychotherapist! (G.E.Vaillant) • Defining the need to drink as related to some psychological pathology ( early trauma, rearing, relations with parents etc) – doomed to fail • Attach to a group or a movement, not an individual when transference issues may well ensue
Claimed detrimental effects of AA • Diminish other treatment effects? Published studies show augmentation of treatment effects • AA is against use of medications? ‘For each alcoholic there may be some specific aspects to recovery, ‘follow your doctor’s advice’ (but concern about use of benzos) • Is group pressure coercion? • ‘Substitute dependence – it’s unhealthy’ • Potential for psychological harm due to discussions ? • Embracing sick role by teaching the concept of life-long addiction
A little evidence for: • ‘Intensive case management’ – helping with housing, job, stabilising finances, more rewarding social life • Offering long term follow-up No evidence for: • ‘counselling’ • ‘support’ • residential treatment • BUT, Rychtarik et al, J Cons Clin Psychol, 2000 • ‘severe problems did better with in-patient treatment’ • ‘low problem severity did better in out-patient’
Links between SHGs and recovery millieu • SHG can be linked to the family friends colleagues social setting. • SHGs may counteract negative effects of social milieu (friends and families who drink) • Development of personal resources to protect against relapse-social bonding ,monitoring, modeling, abstinence orientation, fulfilling activities • Rewarding activities –positive influence on recovery