Download
1 / 1
20 likes | 135 Views
EFFECTIVENESS OF AN EDUCATION PROGRAM FOR FAMILIES WITH CONGENITAL ADRENAL HYPERPLASIA. I. Mitchelhill 1 , J. King 2,3 , M. Fisher 2 , G. Betts 1 1 Department of Endocrinology, Sydney Children ’ s Hospital, Randwick. NSW AUSTRALIA

E N D
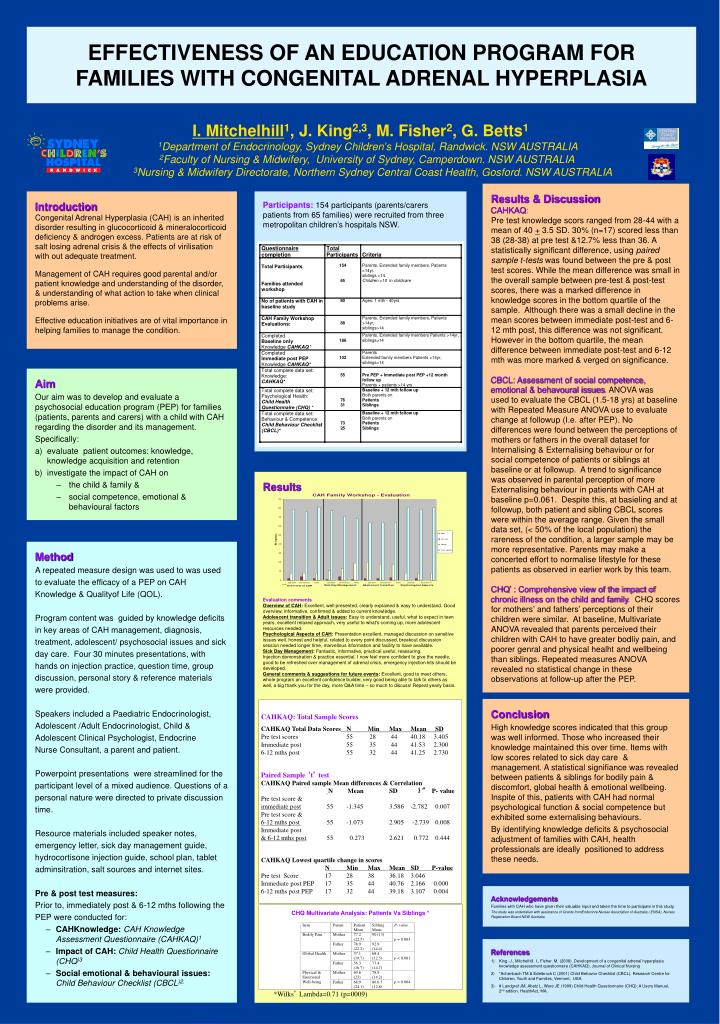
EFFECTIVENESS OF AN EDUCATION PROGRAM FOR FAMILIES WITH CONGENITAL ADRENAL HYPERPLASIA • I. Mitchelhill1, J. King2,3, M. Fisher2, G. Betts1 • 1Department of Endocrinology, Sydney Children’s Hospital, Randwick. NSW AUSTRALIA • 2Faculty of Nursing & Midwifery, University of Sydney, Camperdown. NSW AUSTRALIA • 3Nursing & Midwifery Directorate, Northern Sydney Central Coast Health, Gosford. NSW AUSTRALIA Results & Discussion CAHKAQ: Pre test knowledge scors ranged from 28-44 with a mean of 40 + 3.5 SD. 30% (n=17) scored less than 38 (28-38) at pre test &12.7% less than 36. A statistically significant difference, using paired sample t-tests was found between the pre & post test scores. While the mean difference was small in the overall sample between pre-test & post-test scores, there was a marked difference in knowledge scores in the bottom quartile of the sample. Although there was a small decline in the mean scores between immediate post-test and 6- 12 mth post, this difference was not significant. However in the bottom quartile, the mean difference between immediate post-test and 6-12 mth was more marked & verged on significance. CBCL: Assessment of social competence, emotional & behavoural issues. ANOVA was used to evaluate the CBCL (1.5-18 yrs) at baseline with Repeated Measure ANOVA use to evaluate change at followup (I.e. after PEP). No differences were found between the perceptions of mothers or fathers in the overall dataset for Internalising & Externalising behaviour or for social competence of patients or siblings at baseline or at followup. A trend to significance was observed in parental perception of more Externalising behaviour in patients with CAH at baseline p=0.061. Despite this, at basieling and at followup, both patient and sibling CBCL scores were within the average range. Given the small data set, (< 50% of the local population) the rareness of the condition, a larger sample may be more representative. Parents may make a concerted effort to normalise lifestyle for these patients as observed in earlier work by this team. CHQ* : Comprehensive view of the impact of chronic illness on the child and family. CHQ scores for mothers’ and fathers’ perceptions of their children were similar. At baseline, Multivariate ANOVA revealed that parents perceived their children with CAH to have greater bodliy pain, and poorer genral and physical healht and wellbeing than siblings. Repeated measures ANOVA revealed no statistical change in these observations at follow-up after the PEP. Introduction Congenital Adrenal Hyperplasia (CAH) is an inherited disorder resulting in glucocorticoid & mineralocorticoid deficiency & androgen excess. Patients are at risk of salt losing adrenal crisis & the effects of virilisation with out adequate treatment. Management of CAH requires good parental and/or patient knowledge and understanding of the disorder, & understanding of what action to take when clinical problems arise. Effective education initiatives are of vital importance in helping families to manage the condition. Participants: 154 participants (parents/carers patients from 65 families) were recruited from three metropolitan children’s hospitals NSW. • Aim • Our aim was to develop and evaluate a psychosocial education program (PEP) for families (patients, parents and carers) with a child with CAH regarding the disorder and its management. • Specifically: • evaluate patient outcomes: knowledge, knowledge acquisition and retention • investigate the impact of CAH on • the child & family & • social competence, emotional & behavioural factors Results Evaluation comments Overview of CAH: Excellent, well presented, clearly explained & easy to understand. Good overview, informative, confirmed & added to current knowledge. Adolescent transition & Adult issues: Easy to understand, useful, what to expect in teen years, excellent relaxed approach, very useful to what's coming up, more adolescent resources needed. Psychological Aspects of CAH: Presentation excellent, managed discussion on sensitive issues well, honest and helpful, related to every point discussed, breakout discussion session needed longer time, marvellous information and facility to have available. Sick Day Management: Fantastic, informative, practical useful, reassuring. Injection demonstration & practice essential. I now feel more confident to give the needle, good to be refreshed over management of adrenal crisis, emergency injection kits should be developed. General comments & suggestions for future events: Excellent, good to meet others, whole program an excellent confidence builder, very good being able to talk to others as well, a big thank you for the day, more Q&A time – so much to discuss! Repeat yearly basis. • Method • A repeated measure design was used to was used • to evaluate the efficacy of a PEP on CAH • Knowledge & Qualityof Life (QOL). • Program content was guided by knowledge deficits • in key areas of CAH management, diagnosis, • treatment, adolescent/ psychosocial issues and sick • day care. Four 30 minutes presentations, with • hands on injection practice, question time, group • discussion, personal story & reference materials • were provided. • Speakers included a Paediatric Endocrinologist, • Adolescent /Adult Endocrinologist, Child & • Adolescent Clinical Psychologist, Endocrine • Nurse Consultant, a parent and patient. • Powerpoint presentations were streamlined for the • participant level of a mixed audience. Questions of a • personal nature were directed to private discussion • time. • Resource materials included speaker notes, • emergency letter, sick day management guide, • hydrocortisone injection guide, school plan, tablet • adminsitration, salt sources and internet sites. • Pre & post test measures: • Prior to, immediately post & 6-12 mths following the • PEP were conducted for: • CAHKnowledge:CAH Knowledge Assessment Questionnaire (CAHKAQ)1 • Impact of CAH: Child Health Questionnaire (CHQ)3 • Social emotional & behavioural issues: Child Behaviour Checklist (CBCL)2. Conclusion High knowledge scores indicated that this group was well informed. Those who increased their knowledge maintained this over time. Items with low scores related to sick day care & management.A statistical signifiance was revealed between patients & siblings for bodily pain & discomfort, global health & emotional wellbeing. Inspite of this, patients with CAH had normal psychological function & social competence but exhibited some externalising behaviours. By identifying knowledge deficits & psychosocial adjustment of families with CAH, health professionals are ideally positioned to address these needs. CAHKAQ: Total Sample Scores CAHKAQ Total Data Scores N Min Max Mean SD Pre test scores 55 28 44 40.18 3.405 Immediate post 55 35 44 41.53 2.300 6-12 mths post 55 32 44 41.25 2.730 Paired Sample ‘t’ test CAHKAQ Paired sample Mean differences & Correlation N Mean SD ‘t” P- value Pre test score & immediate post 55 -1.345 3.586 -2.782 0.007 Pre test score & 6-12 mths post 55 -1.073 2.905 -2.739 0.008 Immediate post & 6-12 mths post 55 0.273 2.621 0.772 0.444 CAHKAQ Lowest quartile change in scores N Min Max Mean SD P-value Pre test Score 17 28 38 36.18 3.046 Immediate post PEP 17 35 44 40.76 2.166 0.000 6-12 mths post PEP 17 32 44 39.18 3.107 0.004 Acknowledgements Families with CAH who have given their valuable input and taken the time to participate in this study. The study was undertaken with assistance of Grants fromEndocinre Nurses Association of Australia ( ENSA), Nurses Registraiton Board NSW Australia. CHQ Multivariate Analysis: Patients Vs Siblings * References King. J., Mitchelhill. I., Fisher. M.(2008). Development of a congenital adrenal hyperplasia knowledge assessment questionnaire (CAHKAQ). Journal of Clinical Nursing *Achenbach TM & Edelbrock C (2001) Child Behavior Checklist (CBCL). Research Centre for Children, Youth and Families, Vermont, USA. # Landgraf JM, Abetz L, Ware JE (1999) Child Health Questionnaire (CHQ): A Users Manual, 2nd edition. HealthAct, MA. *Wilks’ Lambda=0.71 (p=0009)