Download
1 / 43
530 likes | 1.41k Views
Pharmacology of Local Anesthesia Part I. Dr. Rahaf Al- Habbab BDS. MsD . Diplomat of the American Boards of Oral and Maxillofacial Surgery 2013. Pain.

E N D
Pharmacology of Local AnesthesiaPart I Dr. Rahaf Al-Habbab BDS. MsD. Diplomat of the American Boards of Oral and Maxillofacial Surgery 2013
Pain Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.
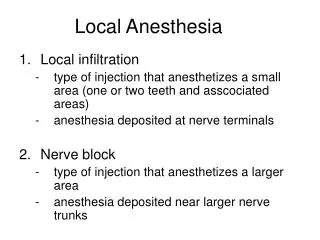
Anaesthesia Anaesthesiais the loss of consciousness and all form of sensation. Local Anaesthesia is the local loss of sensation, disappearing in the following sequence; Pain→ Temperature→Touch→ pressure→ Motor. In dentistry, Only loss of pain sensation is desirable. Local Analgesia.
How Does a Nerve Impulse Occur? Starts with a Stimulus(-90mv_-60mv) → Depolarization of the nerve → Na+ flows from extracellular to Intra-cellular space → Repolarization → K+ flows from Intra-cellular to extra-cellular space
Threshold Potential Normal Local Anesthesia
Between Depolarization and Repolarization, Propagation of the Impulse occur
Local Anesthetic Agents Are drugs that block nerve conduction when applied locally to nerve tissues in appropriate concentrations, acts on any part of the nervous system, peripheral or central and any type of nerve fibres, sensory or motor.
Each Carpule • Local Anesthetic • Vasoconstrictor • Vehicle to make the solution isotonic • Preservative
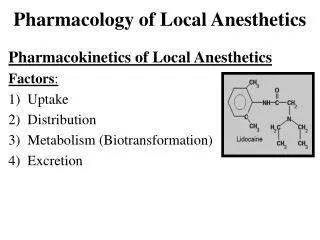
Local Anesthesia Chemistry: They are weak bases, insoluble in water converted into soluble salts by adding Hcl for clinical use. They are composed of three parts: Aromatic (lipophilic) residue with acidic group R1. Intermediate aliphatic chain, which is either ester or amide link R2. Terminal amino (hydrophilic) group R3 and R4. R3 R1COR2 N R4
Mechanism of Action Two Theories • Membrane expansion theory • Specific receptor theory
Mechanism of ActionMembrane expansion theory • A non-specific mechanism similar to the action of general anesthetic agents. • Relies upon the lipophilic moiety of local anesthetic agent. • The molecules of the agent are incorporated into the lipid cell membrane. The resultant swelling produces physical obstruction of the sodium channels, preventing nerve depolarization
Properties of Ideal Local Anesthetic • Possess a specific and reversible action. They stabilize all excitable membrane including motor neurons • Non-irritant with no permanent damage to tissues. • No Systemic toxicity High therapeutic ratio. • Rapid onset and long duration • Active Topically or by injection
Pharmacology of Local AnesthesiaPart II Dr. Rahaf Al-Habbab BDS. MsD. Diplomat of the American Boards of Oral and Maxillofacial Surgery 2013
Classification Classified according to their chemical structures and the determining factor is the intermediate chain, into two groups: Ester Amide They differ in two important aspects: • Their ability to induce hypersensitivity reaction. • Their pharmacokinetics - fate and metabolism.
Ester Class Esters: • Benzocaine • Procaine
Ester Class • Metabolized by Plasma Pseudocholinestrase enzyme, and partially in kidney during excretion. • Allergic reaction to esters: Does not occur to the ester agent but rather to (PABA) • Lead to the formation of Para-Aminobenzoic Acid (PABA)- Highly Allergenic • Some patients have Atypical form of pseudocholinesterase that result in the inability to metabolize esters and therefore induce toxicity.
Amide Class Amides: • Lidocaine • Mepivicaine • Prilocaine • Bupivicaine
Amide Class • Metabolized in the liver • An exception is Prilocaine, where it is metabolized mainly in the liver with some possibility in Lung. • Excreted by Kidneys • Allergy is rare
The kidneys are the primary execratory organ for both types of local anesthesia • Impairment in renal function will result in incomplete removal of local anesthesia and their metabolites from the blood and possibility of toxic reaction
Physiochemical properties These are very important for local anaesthetic activity. Ionization: • They are weak base and exist partly in an unionized and partly in an ionized form. • The proportion depend on: • The pKaor dissociation constant • The pH of the surrounding medium. • Both ionizing and unionizing are important in producing local anaesthesia.
Physiochemical propertiespKa When pKa = pH, there is equal proportion of ionized and unionized form of an agent are present in equal amounts. • The lower the pKa, the more the unionized form, the greater the lipid solubility → Higher the Onset • The higher the pKa, the more the ionized form and the slower the lipid solubility → Lower the Onset
Physiochemical propertiespKa • In general the amide type have lower pKa, and greater proportion of the drug is present in the lipid-soluble (unionized) form at the physiological pH • This produces faster onset of action. • Lidnocaine 1 – 2 minutes (Amide) • Procaine 2 – 5 minutes (Esters) The lower the pKa the faster the onset
Physiochemical propertiesPartition coefficient • This measures the relative solubility of an agent in fat and water. • High numerical value means: • High lipid-soluble • less water-soluble. • More fat solubility, means rapid crossing of the lipid barrier of the nerve sheath. The greater partition coefficient, The faster the onset
Physiochemical propertiesProtein binding • Local anesthetic agents bind with: • α1-acid glycoprotein, which possess high affinity but low capacity. • Albumin, with low affinity but high capacity • The binding is simple, reversible and tend to increase in proportion to the side chain. • Lidnocaine is 64% bound, Bupivacaine is 96% The duration of action is related to the degree of binding. Lidnocaine 15 – 45 minutes, Bupivacaine 6 hours
Physiochemical propertiesVasodilatation ability • Most Local anaesthetics possess a vasodilatory action on blood vessels except Cocaine. • It influence the duration of action of the agent. • Prilocaine is 50% bound to proteins but has a longer duration than Lidnocaine (64%) since it possess no strong vasodilatory effect. Affect the duration of action of the agent
Summary • Rapid Onset: • Low pKa value– more unionized – Amides • Higher Partition coefficient – more lipid soluble • High PH • Long duration of action: • High protein binding. • Low vasodilatation property.
Pharmacology of Local AnesthesiaPart III Dr. Rahaf Al-Habbab BDS. MsD. Diplomat of the American Boards of Oral and Maxillofacial Surgery 2013
Local Anesthesia Local Anesthetic Concentration Vasoconstrictor Concentration 1:20 000=0.05 mg/ml (50mcg/ml) 1:50 000=0.02mg/ml (20mcg/ml) 1:100 000=0.01mg/ml (10mcg/ml) 1:200 000=0.005mg/ml (5mcg/ml) 0.5%=5mg/ml 1.0%=10mg/ml 2.0%=20mg/ml 3.0%=30mg/kl 4.0%=40mg/ml Note: Each Carpule contains 1.8 cc Therefore 1 carpule of 2% drug with 1:100 000 Vasoconstrictor contains 36mg of Drug 0.018mg or 18mcg of vasoconstrictor
How to calculate the maximum dose of L.A? • Multiply patients weight (kg) by the maximum dose of the L.A • Divide the result by the L.A value • (1.8x20=36 in 2% lidocaine) Example: Calculate the maximum dose of 2% Lidocaine with 1:100 000 epi, in a 150 lbs patient: • 150 ÷ 2.2 = 68kg • 68 x 7 = 477mg • 477 ÷ 36 = 13.25 Cartridge
Vasoconstrictors • Originally added to reduce systemic uptake in an attempt to limit toxicity • Prolong the duration • Produces profound anaesthesia. • Reduce operative bleeding. • Two types: • Sympathomimetic naturally occurring. • Synthetic polypeptides, Felypressin
Epinephrine(Adrenaline) • Hormone and Neurotransmitter released from the Adrenal Gland, act on Adrenergic receptors. • Has both Alpha and Beta activity, affecting α1, α2, β1, β2 and β3 • Uses in dentistry: • Local anaesthetic solution. • Gingival retraction cords. • In the ER as life-saving drug in anaphylaxis. • Mechanism of action: • Interact with adrenergic receptors in the vessels and muscles: • α1 & α2 producing vasoconstriction in skin & MM • β2 stimulation causing vasodilatation in skeletal muscles.
Vasoconstrictors Systemic effect Being a naturally occurring hormone, it exert a number of physiological responses on the different systems; The heart: Has direct and indirect action. • Direct action on β1receptors increases the rate and force of contraction raising cardiac output. • Indirect action, increase pulse and cardiac output, lead torise in systolic blood pressure, (not with dental dose)
VasoconstrictorsSystemic effect Blood vessels: Contain α1,α2andβ2 adrenoreceptors in the vessels of the skin, mucous membrane and skeletal muscles. α1 receptors causes vasoconstriction since they are susceptible to endogenous nor-epinephrine and exogenous epinephrine. Reduce operative bleeding
VasoconstrictorsSystemic effect Haemostasis: • The vasoconstriction effect. • Adrenaline promote platelets aggregation in the early stages. Lungs: • Stimulation of β2 receptors in the lung lead to bronchial muscle relaxation, life-saving in bronchial (spasm) • constriction during anaphylactic reaction.
Systemic EffectSummery • Vasoconstriction (α1) • Increase Heart Rate (β1) • Increase Cardiac Output (β1) • Decrease Blood Pressure (α2) (β2 effect in skeletal muscles) • Bronchodilatation (β2 effect on smooth muscles)
Local Anesthesia ToxicityCauses • Accidental IV administration • Overdose
Local Anesthetic Toxicity Risk Factors Geriatric (Pediatric): • Slower metabolism • Multiple medications can cause adverse drug reaction Cimitidine medication: • Histamine H2-Receptor Antagonist, inhibits P-450 (Hepatic oxidative enzyme) needed for metabolism, causes accumulation of local anesthetic Propranolol or β-blockers: • Decrease hepatic blood flow decreasing L.A clearance Administration of Opioids with L.A: Increases sensitivity
Local Anesthesia ToxicitySigns and Symptoms CNS Effects: • L.A readily crosses the BBB • Usually first S/S or overdose are CNS related • Spectrum of activity with increasing dose. CVS Effect: • More resistant than CNS so appears later • At toxic doses LA causes depression of myocardium and decreased SVR