Download
1 / 209
2.12k likes | 2.3k Views
Biostatistics. Primary MMed (Anaesthesia). Writing a study protocol. introduction research question current knowledge research hypothesis research objective. Writing a study protocol. methodology type of study experiments prospective (randomized, control) observational prospective

E N D
Biostatistics Primary MMed (Anaesthesia)
Writing a study protocol • introduction • research question • current knowledge • research hypothesis • research objective
Writing a study protocol • methodology • type of study • experiments • prospective (randomized, control) • observational • prospective • retrospective • audit
Writing a study protocol • methodology • sample size calculation • guided by expected difference in either proportion or numerical data, standard deviation of known data, α and β values, and intended power of study • plan to recruit more subjects in case of drop outs • size of drop outs will affect the basis of assumptions and the initial sample size calculation, and the research hypothesis may show no significant difference (P>0.05)
Writing a study protocol • methodology • patient consent • inclusion criteria • exclusion criteria, restriction • process of randomization • procedure (how to go about carrying out the data collection) • control group • test group(s)
Writing a study protocol • methodology • monitoring of the patients during the period of procedure • routine - heart rate, blood pressure, oxygen saturation • data / observations • side effects of test protocol • rescue therapy • safety of patient • treatment plan • criteria for withdrawal from study
Writing a study protocol • statistical analysis • the data will be subjected to a test for normality • statement about treatment of normal or nonparametric distribution of data • normal distribution • expressed as mean and standard deviation, with 95% confidence interval • t-test for comparison of means obtained from 2 groups of data • analysis of variance test for comparison of means obtained from more than 2 groups • Χ2 test for discrete data
Writing a study protocol • statistical analysis • non-normal distribution • expressed as median and range, with limits of 25th and 75th percentiles • Mann-Whitney U test for analysis of data from 2 groups • Kruskal-Wallis test for analysis of data from more than 2 groups • state the P value and decide on the significance level, conventionally it is P<0.05 • submit protocol for ethics committee approval
Null hypothesis • study hypothesis • investigator conducting a study usually has a theory in mind • however, very difficult to prove the hypothesis • simpler to disprove a hypothesis than proving it • null hypothesis • differences observed is not due to exposure to factor, and is by chance • always phrased in the negative and that is why it is termed null
Types of research Longitudinal studies Cross-sectional studies
Types of research - longitudinal study • investigates a process over time • the effect of external factors on human subjects • 3 types • clinical trial, a cohort study, case-control study • prospective or retrospective studies • in prospective studies, subjects are grouped according to ‘exposure’ to some factor • in retrospective studies, subjects are grouped according to outcome, the ‘exposure’ effect is then determined retrospectively
Types of research - cross-sectional study • describes a phenomenon fixed in time • description of staging system for cancer • laboratory studies of biological processes
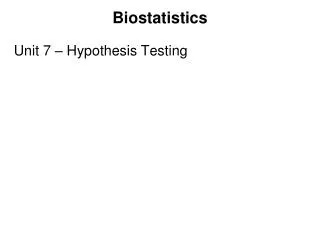
longitudinal studies prospective studies according to “exposure” randomised non-randomised observational studies retrospective studies according to outcome determine “exposure” cross sectional studies disease description diagnosis and staging abnormal ranges disease severity disease processes Comparison
Randomised clinical trial • randomisation • is a procedure in which the play of chance enters into the assignment of a subject to the alternatives (control and test groups) under investigation, so that the assignment cannot be predicted in advance • tends to produce study groups comparable in unknown as well as known factors likely to influence outcome apart from the actual treatment being given itself • guarantees that the probabilities obtained from statistical tests will be valid
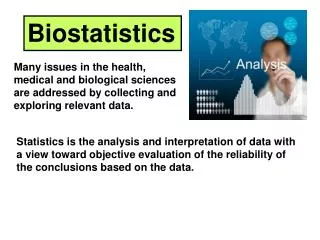
Randomised clinical trial - designs • parallel designs • one group receives the test treatment, and one group the control • cross-over designs • the subjects receive both the test and the control treatments in a randomised order • each subject acts as own control, allowing paired or matched analysis, and provides an estimate of the difference between test and control • useful in chronic disease that remain stable over time, such as diabetes and asthma, where the purpose of treatment is palliative, not cure
Designs of a randomised clinical trial: parallel, cross-over Test Assessment Randomisation Control A parallel design clinical trial Test Control Assessment Assessment Randomisation Control Test A two period cross-over design clinical trial
Problems of cross-over design • cross-over effect • possibility that the effect of the particular treatment used in the first period will carry over to the second period, and may interfere with how the treatment scheduled for the second period will act, thus affecting the final comparison between the two treatments • to allow for this possibility, a washout period, in which no treatment is given, should be included between successive treatment periods
Problems of cross-over design • disease may not remain stable over the trial period • subject drop-outs • more will occur in this design trials than in parallel design trials, due to extended treatment period
Non randomised studies • historical controls • when randomisation is not possible • problem of bias selection already occurring - those who did not receive transplants may be more ill or may not have satisfied the criteria • survival of patients who received heart transplants and patients who did not
Non randomised studies • pre-test–post-test studies • a group of individuals are measured, then subjected to treatment or intervention, and then measured again • purpose of the study is to study the size of the effect of treatment or intervention (e.g. campaign) • major problem is ascribing the change in measurement to the treatment since other factors may also have changed in that interval
Cohort • a cohort is a component of a population identified so that its characteristics can be ascertained as it ages through time • designated groups of persons either born in a certain year or traced over a period of time (who ever worked in a factory)
Cohort studies • cohort study • one in which subsets of a defined population can be identified who have been exposed (or will be exposed) to a factor which may influence the probability of occurrence of an outcome (given disease) • usually confined to studies determining and investigating aetiological factors and do not allocate the equivalent of treatments • also for post-marketing surveillance, comparing adverse effects of new drug with alternative treatment • may be referred to as follow-up, longitudinal or prospective study • often termed observational studies, since they observe the progress of individuals over time
Progress of a cohort study With disease With disease Exposed Population Without disease Without disease With disease Not exposed Without disease Time
Problems with cohort study • exposure to factor may be by natural selection or up to the individuals’ decision • bias may influence the measure of interest • other associated factors may also influence measure of interest • e.g. cohort study of cardiovascular risk in men sterilised by vasectomy • e.g. incidence of breast cancer with consumption of alcohol
Problems with cohort study • size of the study • the required size of a cohort study depends not only on the size of the risk being investigated but also the incidence of the particular condition under investigation • cohort studies not suitable for investigating aetiological factors in rare diseases
Problems with cohort study • problems with interpretation • bias pool of study subjects • when cohort is made up of employed individuals, the risk of dying in the first few years of follow up is less than in general population, this is known as healthy worker effect; people who are sick are less likely to be employed • incomplete representation • e.g. people who respond (to questionnaires) and people who are lost to follow up
Case-control studies • case-control study • also known as a case-reference study or retrospective study • starts with identification of persons with the disease (or other outcome variable) of interest, and a suitable control group of persons without the disease • the relationship of a risk factor to the disease is examined by comparing the two groups with regard to how frequently the risk factor is present
Case-control studies Exposed Subjects with disease (case) Not exposed Exposed Subjects without disease (control) Not exposed Time (Retrospective)
Case-control studies • designs • matched design • control subjects can be chosen to match individual cases for certain important variables such as age, gender and weight • unmatched design • controls can be a sample from a suitable non-diseased population
Case-control studies • selection of controls • not required that the control group are alike in every aspect to the cases, usually 2 or 3 variables which presumably will influence outcome are matched, such as age, gender, social class • main purpose is to control for confounding variables that might influence the case-control comparison • confounding arises when the effects of two processes are not separated, e.g. disease related to 2 exposure factors
Case-control studies • selection of controls • matching can be wasteful if matching criteria leads to many available controls being discarded because they fail the matching criteria • if controls are too closely matched to their respective cases, the relative risk may be underestimated
Limitations of case-control studies • ascertainment of exposure relies on previously recorded data or on memory, and it is difficult to ensure lack of bias between the cases and controls • the cases may be more motivated to recall possible risk factors • difficulty with selection of suitable control group • a major source of criticism
Cross-sectional studies • subjects are included without reference to either their exposure or their disease • usually deals with exposures that do not change, such as blood type, or chronic smoking habit • resembles a case-control study except that the number of cases are not known in advance, but are simply the prevalent cases at the time of survey
Cross-sectional studies • sampling methods • quota sample • to ensure that the sample is representative of general population in say, age, gender and social class structure • not recommended in medical research • grab or convenience sample • only subjects who are available to the interviewer can be questioned
Cross-sectional studies • problems • bias in the type of responders and non-responders • exposures have to be determined by a retrospective history
Calculation of sample size • consider • control group response • the anticipated benefit (of the treatment) • significance level • power
Control group response • it is first necessary to postulate the response of the control group patients • denoted by π1, to distinguish it from the value that will be obtained from the trial, denoted p1 • experience of other studies may provide π1
The anticipated benefit • it is also necessary to postulate the size of the anticipated response in treatment group patients, denoted by π2, to distinguish it from the value that will be obtained from the trial, denoted p2 • anticipated benefit δ = π2 - π1
Type I error • the error of incorrectly rejecting the null hypothesis when it (the hypothesis) is true • the error of concluding that the differences seen in the result is significant when in fact it is not • wrongly accepting that differences in the results as significant when there is no difference • designated α • equivalent to the false positive rate (1-specificity)
One or two-sided • null hypothesis (H°) is that there is no significant difference, and chance has occurred • no assumption about the direction of change or variation • alternate hypothesis states that the difference is real, further that it is due to some specific factor, • where no direction of change is specified both ends of the distribution curve are important, and the test of significance is two-sided, or two-tailed • where the direction is specified, then only one tail of the curve is relevant, and the test of significance is one-sided, or one-tailed
One or two-sided • the critical value is the value of a test statistic at which we decide to accept or reject H° • critical value for a one-sided test at significance p, will be equivalent to that for a two-sided test at 2p • one-sided p = 0.025 / two-sided p = 0.05 • thus, it is tempting to use one-sided tests as the significance is greater, but the decision should be made before the data is collected, not after the direction of change is observed and should be clearly stated when presenting results
One or two-sided Frequency μ = 0 P<5% (two-sided) P<2.5% (one-sided) 1.96σ z
Significance level • the significance level, α, is the probability of making a Type I error and is set before the test is carried out • in most cases, it will be two-sided
Significance level • denoted by the letter P, represents the probability of the observed value being due solely to chance variation • can be interpreted as the probability of obtaining the observeddifference, or one more extreme, if the null hypothesis is true • the smaller the value of P, the less likely the variation is to be due to chance and the stronger the evidence for rejecting the null hypothesis
Significance level • most scientific work, by accepted convention, rejects the null hypothesis at P < 0.05 • probability of the observed value being due solely to chance is < 0.05 (or < 1 in 20) • this means that we shall reject the null hypothesis on 5% of occasions, when it is in fact true, i.e. there was simply a chance variation and that the 2 treatment are equally effective
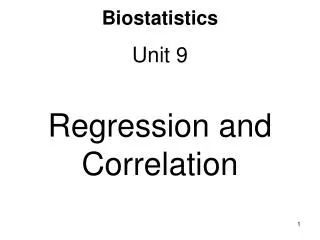
α the probability that a random variable, (Normally distributed with mean = 0 and standard deviation = 1) will be greater than z or less than -z z the value on the horizontal axis of a Normal distribution corresponding to the probability α α/2 α/2 –zα +zα Significance levels
Significance level • if α is 0.05, then the corresponding z is 1.96 • to link z with the corresponding α, we write z0.05 = 1.96 • zα is the value along the axis of a Normal distribution • thus • 0.05/2 = 0.025 is to the left of z = –1.96 • 0.025 is to the right of z = +1.96
Type II error • error in incorrectly accepting the null hypothesis of no difference between treatments, when it (the hypothesis) is in fact false (and should be rejected) • accepting the null hypothesis when there should be significant difference in the results • accepting that the differences seen in the result is not statistically significant and making the conclusion P>0.05 • the probability of making a type II error is designated β • equivalent to the false negative rate (1-sensitivity)