Download
1 / 40
460 likes | 816 Views
CAROTID ARTERY DISEASE. Epidemiology. 3 rd most common cause of death in the US Most common cause of long term disability 500,000 CVAs annually Contributes 200,000 deaths annually Of those that survive, 2/3 have disability, 1/3 require hospitalization for it. 16 trillion$ a year in costs .

E N D
Epidemiology • 3rd most common cause of death in the US • Most common cause of long term disability • 500,000 CVAs annually • Contributes 200,000 deaths annually • Of those that survive, 2/3 have disability, 1/3 require hospitalization for it. • 16 trillion$ a year in costs
Risk Factors Nontreatable • Age • Ethnicity • Gender • Family History • Genetics
Hypertension TIA’s Previous CVA’s Asx Bruit or Stenosis Cardiac Disease Aortic Arch atheromatosis Diabetes Mellitus Cigarette Smoking ↑fibrinogen, ↑homocysteine ↑anticardiolipin Oral contraceptives Obesity Risk FactorsTreatable
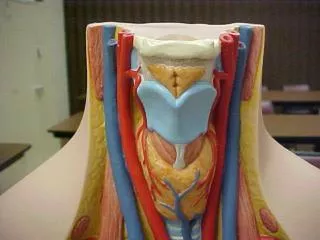
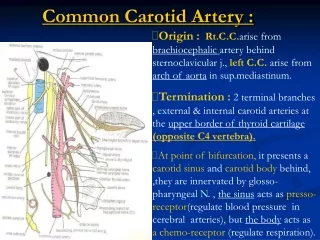
Anatomy • Brain 2% of body weight but 17% of CO and 20% of O2 supply….so neural tissue can become necrotic within minutes • Branches of aortic arch; inominate (Brachiocephalic), L common carotid and L subclavian.
Anatomy • Inominate branches to form R subclavian and R common carotid. • 10% of population L common comes of inominate.
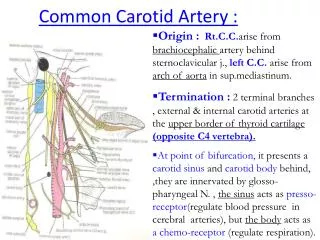
Anatomy • Brain supplied by 2 internals and 2 vertebrals. The internal supply 80-90% of total blood flow. • The common carotids bifurcate at angle of mandible into external and internal. • Branches if external are lingual, ascending pharyngeal, superior thyroid, occipital, posterior auricular. The terminal branches are int. maxillary and superficial temporal a.
Anatomy • Extensive collaterals between external and vertebrals in case of occlusion • Periorbital collaterals connect through ophthalmic artery to internal carotid in case of occlusion in neck. • Extensive side to side collaterals between L and R externals and L and R vertebrals.
Anatomy • Internals branch into anterior cerebral and middle cerebral arteries • The L and R middle cerebrals connect at the circle of Willis via anterior and posterior communicating arteries. • 15% have no connections between ant and post cerebral circulations, 35% lack connection between the two hemispheres.
Anatomy • Vertebrals arise from first portion of subclavian artery and enter 6th cervical vertebra and ascend in foramen. Unite to form Basilar artery. The Basilar terminates as L and R posterior cerebral arteries posterior communicating arteries of the circle of Willis.
Anatomy • Branches of external carotid can anastamose with orbital arteries supply internal carotid artery in case of proximal occlusion • Collateral between external and ophthalmic are most important of these.
Anatomy • Vertebral gives off branches to muscles of neck…if proximal vertebral gets occluded, the external can supply the distal vertebral via these branches. • If common occluded, blood can go from vertebral to external branches to internal • Finally branches of the L and R external can anastamose freely across the face.
Pathophysiology • Complication of atherosclerosis (most common) • High shear stress (bifurcations) • Intimal injury • Carotid bulb plaques • Aneurysms, kinks, coiling…. • FMD (thickened,beaded), Takayashu (women, branches of aorta) arteritis, Temporal arteritis (elderly, blindness). • Trauma
Atherosclerosis • Locations of turbulence, like bifurcations • The common carotid is most common spot in the cerebral circulation • Occur along the outer wall of bifurcation, and only proximal portion of external.
Atherosclerosis • At bifurcation you get separation of flow, disruption of laminar flow, flow stasis, prolonged residence time, shear stress • Grossly the plaque is thickest at the bifurcation, extending 2cm into distal internal carotid.
Atherosclerosis • The plaque occupies the media and intima, sparing the outer media and adventitia. • The plaque tapers from the media into the normal intima. • Mature plaques are characterized by a heterogeneous core and fibrous cap. Disruption of the cap leads to embolization and thrombosis. Also exposes the non-endothelized intima to platelets (ulcer).
Plaque Composition • Fibroblast proliferation • Lipid accumulation • Calcification • Ulceration • Sub-intimal hemorrhage • Thrombosis
Clinical Presentation • TIA: resolves within 24h. Can present as a transient hemispheric event or monocular blindness (amaurosis fugax). A hemispheric attack presents with contralateral combined sensory and motor deficit or purely motor or purely sensory deficit.
Clinical Presentation • When ischemia occurs in the posterior circulation, it causes vertebrobasilar insufficiency presenting as vertigo, drop attacks, binocular vision loss, dysarthria, dysphagia, incoordination. • A stroke lasts more than 24h. Most are a result of emboli to branches of middle cerebral artery
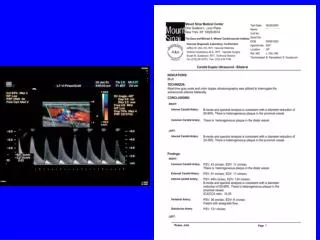
Evaluation • Physical Exam • Duplex (most accurate in >50% stenosis) • MRA • Angiography (gold standard, but risks)
Duplex • Excellent screen for neurologic sympt. • peak sys. Velocity > 220cm/sec • end dias. Velocity > 80cm/sec • post stenotic turbulence • Less reliable in anatomic variants • Operator dependant
Carotid Angiography • Gold Standard • Remains the most definitive tool for decision to operate • Complications ~ 1-4% • Pseudoaneurysm • Stroke • Dissection
Natural History- Symptomatic Dz • Cumulative risk for stroke at 5 years after a TIA is 30-50%. • 1/3 patients die within 5y of TIA, usually of CAD. • Risk for stroke following TIA 10-30% in first year, 6% risk subsequent years. • After stroke, a 20-30% mortality, risk of recurrent is 5-40%, with 30% of these fatal.
Asymptomatic Disease • Only 10% of stroke patients have had a TIA prior. • Asymptomatic bruits are present in 5% of population>50 • Bruits are not diagnostic of significant stenosis. (only 23% have >50% stenosis)
Asymptomatic Disease • Risk of stroke is proportional to degree of stenosis (greatest over 80% stenosis) • For patients with 75-80% stenosis, risk of stroke 18-46%.
Asymptomatic Disease • Risk of stroke elevated in patients undergoing major surgical procedures such as CABG, vascular surgery. • Stroke is not increased with unilateral asymptomatic high grade carotid disease during CABG, but it is in bilateral high grade stenoses.
Medical Treatment • Control risk factors • No drug therapy has been shown to reduce the risk of stroke in asymptomatic disease.
Medical Treatment • No study has provided definitive evidence that systemic anticoagulation reduces the risk of stroke in patients who have had a stroke or TIA. • ASA has been shown to decrease the morbidity and mortality from symptomatic disease • In patients with TIA or stroke, ASA demonstrated a 22% risk reduction in recurrent strokes, TIA, MI, or vascular death, compared with controls. • Plavix and ASA offers no added benefit.
Symptomatic Disease • Degree of ICA stenosis is most important predictor of CVA • Severity of stenosis is proportional to Risk of Stroke • Definite benefit of surgery in symptomatic pts with > 70% stenosis is established in three major studies (NASCET, ECST, VATCE)
NASCET north american symptomatic carotid endarterectomy trial • Double armed, prospective trial • Medical vs. Surgical therapy • Pt.s developing sx.s during the trial were operated and excluded • 5 yr trial terminated at two years due to end point • Surgery 9%, Medical 26%
NASCET (cont.) • Risk of major CVA was ↓ by 80% at 2yr follow-up. • CEA was beneficial in symptomatic pts with occlusion of contralateral carotid.
ECST european carotid surgery trial • Double armed prospective trial, 3y f/u • Medical vs. Surgical therapy • 70-99 % stenosis • 778 pts with carotid distribution CVA, TIA or retinal infarction • Surgery 12.3%, medical 22%
VATCE veterans affairs trial of carotid endarterectomy • Terminated early due to early endpoints in NASCET and ECST trials. • Also showed Carotid Endarterectomy to be beneficial in symptomatic patients. • Surgery 7%, medical 20%
Symptomatic Trials: Summary • 0-29% CAS- medical therapy with anti-aggregate platelet therapy • 30-69% CAS- medical therapy probably desirable in most patients* • 50-69%- CAS- surgery provides modest benefit in hemispheric ischemia • ≥ 70% CAS- surgical therapy indicated
Asymptomatic Disease • Prevalent in the elderly population • Asymptomatic CAS >70% rare • Asymptomatic bruit 1.5% risk of CVA per year X 5 yr.s • <75% ~ 1.3%/yr. • >75% ~ 10.5%/yr.
CASANOVA carotid artery surgery asymptomatic narrowing : operation vs. aspirin • Asymptomatic pt.s with CAS 50-90% • Prospective double armed trial • Medical therapy (330 mg ASA QD + 75mg dypyridamole TID) • Surgical therapy- CEA
CASANOVA (cont) • No statistically significant difference in medical vs. surgically treated groups.
ACAS asymptomatic carotid atherosclerosis study • CEA, ASA and medical risk factor mgmt in patients < 80y/o with CAS>60% • Risk of CVA reduced over 5 yrs by 5.9% • Absolute yearly reduction of 1% • Benefit negated by many factors.
Asymptomatic Trials: Summary • Asymptomatic patients with CAS > 80% will benefit from surgery assuming the surgeon has complication rate <3% • Some investigators refrain from recommending surgery in any asymptomatic patient.
Endovascular Treatment • Problem of embolization from angioplasty • Use of cerebral embolic protection devices • 4 prospective randomized trials comparing endo and surgery. 3 were in adequate risk, 1 in high risk only. CAVATAS, Wallstent, Sapphire (only one with protection device), the other was stopped 5/7 stroked after stenting! • Long-term efficacy and durability is unknown. • At present limited to high risk only