Download
1 / 26
350 likes | 1.96k Views
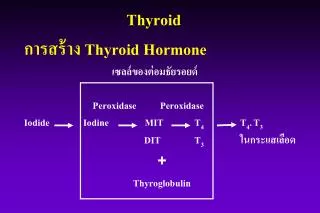
Thyroid. การสร้าง Thyroid Hormone เซลล์ของต่อมธัยรอยด์ P eroxidase Peroxidase Iodide Iodine MIT T 4 T 4 . T 3 DIT T 3 ในกระแสเลือด + Thyroglobulin. Metabolism of TH.

E N D
Thyroid การสร้าง Thyroid Hormone เซลล์ของต่อมธัยรอยด์ Peroxidase Peroxidase Iodide Iodine MIT T4 T4.T3 DIT T3 ในกระแสเลือด + Thyroglobulin
Metabolism of TH T3 - 80% T3 ในกระแสเลือด, active form Reverse T3 (inactive form) 5’ monodeiodination T4 5 monodeiodination
Hypothalamus TRH + - Pituitary Peripheral Tissue - TSH + Thyroid TBG - T3 TBG - T4 T4,T3 + TBG
I. ความผิดปกติของการทำงานของต่อม thyroid - Thyrotoxicosis / Hyperthyroidism - Hypothyroidism II. ต่อมธัยรอยด์ thyroid ทำงานปกติ แต่มีขนาดโตขึ้น - Diffuse euthyroid goiter - Solitary thyroid nodule - multinodular goiter III. ความผิดปกติของ thyroid function test โดยที่ต่อม thyroid ทำงานผิดปกติ - Euthyroid hyperthyroxinemia - Euthyroid sick syndrome - Euthyroid hypothyroxinemia Thyroid disorder
Thyrotoxicosis - ภาวะที่ thyroid hormone ในเลือดสูง - ต่อมสร้าง hormone มาก - มีการทำลายต่อม ต่อมปลาย thyroid H. มาก อาการ : เหนื่อย, ใจสั่น, นน.ลด, กินเก่ง, ขี้ร้อน, เหงื่อออกมาก ขี้โมโห, หงุดหงิด, ผมร่วง, ท้องเดิน, ประจำเดือนผิดปกติ
อาการแสดง Fine tremor, moist skin & warm tachycardia, hyperactive Plummer’s Nails Staring eyes, Lid retraction, Lid Lag Localized myxedema (pretibial)
สาเหตุ - Graves’ disease - Toxic multinodular goiter - Toxic Adenoma - Thyroiditis - Struma Ovarii - Functioning metastatic thyroid CA - Thyrotoxic factitia - Hydatidiform mole Diagnosis : TH , TSH (<0.1)
TBG เพิ่มขึ้น TBG ลดลง ตั้งครรภ์ มีการเจ็บป่วย (major systemic illness) ทารกหลังคลอด กลุ่มอาการเนโฟรติค มีภาวะเอ็สโตรเจนมากเกิน ภาวะทุพโภชนาการ ได้รับเอ็สโตรเจน active acromegaly ได้รับยาคุมกำเนิด ได้รับฮอร์โมนเพศชาย ได้รับเฮโรอีนได้รับยา tamoxifen ได้รับยากลูโคคอร์ติคอยด์ในขนาดสูง ได้รับยา perphenazine ได้รับยา L-asparaginase ติดเชื้อโรคเอดส์ พันธุกรรม Chronic active hepatitis Biliary cirrhosis Acute intermittent porphyria พันธุกรรม ตารางที่ 3 ภาวะที่ทำให้ระดับซีรั่ม TBG ผิดปกติ
สาเหตุของภาวะธัยรอยด์ฮอร์โมนเป็นพิษ ลักษณะเฉพาะทางคลินิกสาเหตุของภาวะธัยรอยด์ฮอร์โมนเป็นพิษ ลักษณะเฉพาะทางคลินิก associate with hyperthyroidism มีค่า radioactive iodine uptake(RAIU) สูง Graves’ disease ต่อมธัยรอยด์โตแบบทั่วไป และฟังได้เสียง bruit, ophthalmopathy, dermopathy Toxic multinodular goiter มีการจับ radioiodine ที่ nodule หลายแห่ง Toxic adenoma มีการจับ radioiodine ที่ nodule Hashimoto’ disease (Hashitoxicosis) ตรวจพบซีรั่ม TPOAb และ/หรือ TgAb ในระดับสูง Thyrotropin producing pituitary tumor มีก้อนเนื้องอกที่ต่อมใต้สมอง, ระดับซีรั่ม T4 สูง ร่วมกับระดับซีรั่ม TSH ปกติหรือสูง Hydatidiform mole ตรวจพบระดับซีรั่ม HCG ปกติหรือสูง ตารางที่ 1 สาเหตุและลักษณะเฉพาะทางคลินิกของภาวะธัยรอยด์ฮอร์โมนเป็นพิษ และฮัยเปอร์ธัยรอยดิสซึม
สาเหตุของภาวะธัยรอยด์ฮอร์โมนเป็นพิษ ลักษณะเฉพาะทางคลินิกสาเหตุของภาวะธัยรอยด์ฮอร์โมนเป็นพิษ ลักษณะเฉพาะทางคลินิก ที่ไม่มีฮัยเปอร์ธัยรอยดิสซึม มีค่า RAIU ต่ำ Thyroid hormone therapy ระดับซีรั่ม thyroglobulin ต่ำ Thyrotoxicosis factitia ระดับซีรั่ม thyroglobulin ต่ำ Subacute thyroiditis ต่อมธัยรอยด์มีขนาดใหญ่ขึ้นและเจ็บ, มีค่า ESR สูง Lymphocytic (silent) thyroiditis ต่อมธัยรอยด์มีขนาดใหญ่ขึ้นแต่ไม่เจ็บ และตรวจพบ TPOAb Postpartum thyroiditis ต่อมธัยรอยด์มีขนาดใหญ่ขึ้นแร่ไม่เจ็บ และตรวจพบ TPOAb ในระยะ 6 เดือนแรก หลังคลอดบุตร
แยกโดย radioactitive iodine uptake (RAIU) RAUI ปกติหรือสูง Graves’ disease Toxic multinodular goiter Toxic adenoma Hydratidiform mole TSH producing tumor Pituitary resistance ต่อ thyroid hormone ตารางที่ 3. แสดงสาเหตุของภาวะธัยรอยด์ฮอร์โมนเป็นพิษ
RAUI ต่ำ Transient painless thyroiditis subacute painful thyroiditis Hashimoto’s thyroiditis Strum ovarii Thyrotoxic factitia Iodine induce thyrotoxicosis Funcfioning metastatic follicular carcinoma
1. Medication 2. I131 therapy 3. Surgery Medication - อายุน้อย - อาการไม่มาก - ขนาดของต่อมไม่โต Thionamide- propylthiouracil (PTU) - Methimazole (MMI) การรักษา
1. inh. oxidation ของ iodine ในการจับกับ tyrosine residues บน thyroglobulin 2. inh. การรวมตัวของ MIT, DIT 3. inh. การเปลี่ยน T4 เป็น T3ที่ peripheral tissue 4. ลดระดับ TSI *MMI และ CBZ ไม่มี 3. Dose : PTU 150- 300 mg/d MMI 15- 30 mg/d Duration 1 1/2 -2 yrs. Action
PTU & MMI - Pregnancy, lactation PTU - Thyroid crisis PTU - Surgery MMI , PTU rectal suppository
ตารางที่ 4 คุณสมบัติทางเภสัชวิทยา และผลไม่พึงประสงค์ของยาต้านธัยรอยด์ PTU MMI Serum protein binding ~75% nil Serum half-life 75 นาที ~4-6 ชั่วโมง Volume of distribution ~20 ลิตร ~40 ลิตร Metabolism of drug illness Severe liver disease ปกติ ลดลง Severe kidney disease ปกติ ปกติ
PTU MMI Transplacental passage น้อย มากกว่า Levels in breast milk น้อย มากกว่า Potency 1 10 Inhibition of peripheral - ไม่มี conversion of T4 to T3 All adverse reactions 7.1% 3.3% Magor adverse reactions Agranulocytosis 0.4%(idiosyncrasy) 0.1%(dose related) Hepatotoxicity hepatocellular damage cholestasis Vasculitis พบบ่อยกว่า พบน้อยกว่า
rash, itching alopecia, arthralgia, fever *agranulocytosis hepatitis, thrombocytopenia vasculitis, pneumonitis SE
Hypothyroidism - ภาวะที่มีระดับ thyroid H. ในเลือดต่ำ อาการเฉื่อยชา, ขี้เกียจ, เชื้องช้า, ท้องผูก, ขี้หนาว ผิวหนังแห้ง, ประจำเดือนผิดปกติ อาการแสดง Bradycardia, Slow reflex relaxation coarse skin & dry hoarseness, edema Lab : T4 TSH - 1O Hypothyroidism
O สาเหตุของ 1 Hypothyroidism - ขาด iodine - ได้รับ goitrogen - Hashimoto’s thyroiditis - ความผิดปกติของ enzyme ในการสร้าง TH การรักษา - Na - L - thyroxine 0.1 - 0.15 mg/d oral form - iodine supplement
ก้อน + TH, TSH ปกติ 10-20 yrs. TH ปกติ, TSH. (autonomous hyperfunction) Toxic Multinodular goiter Treatment - Surgery - I131 Therapy Multinodular goiter
Solitary Thyroid Nodule - Benitgn or Malignancy - HX & PE - FNA & Biopsy - Other : thyroid Scan - cold nodule - hot nodule : ultrasound - Treatment - FNA - Benign Na-L-thyroxine Suppressive dose
Diffuse Euthyroid goiter สาเหตุ 1. Hashimato’s thyroiditis 2. Iodine deficiency 3. ได้รับ goitrogen 4. ความผิดปกติของ enzyme 5. physiologic - puberty - pregnancy 6. Idiopathic Diagnosis : TH & TSH ปกติ Treatment : Na-L-thyroxine suppressive dose 0.15-2.0 mg/d
DIFFUSE ENLAEGEMENT OF THYROID GLAND ประวัติ ตรวจร่างกาย บ่งชี้ว่าเป็น hyperthyroidism บ่งชี้ว่าเป็น hypothyroidism หรือ euthyroid T3 (หรือ FT3) TSH T4 (หรือ FT4) TSH T3 สูง TSH ต่ำ T4,T3 ปกติ TSH ปกติ T4 ต่ำ TSH สูง EUTHYROID GOITER HYPOTHYROIDISM HYPERTHYROIDISM
HYPERTHYROIDISM Multinodular Nodule Diffuse Hot nodule หรือ GRAVES’ ร่วมกับ cold nodule Toxic multinodular goiter เพิ่งโต ไม่มี eye sign อาการน้อย โตมานาน + exophthalmos หรือ localized myxedema ดูต่อในแผนภูมิ thyroid nodule 131I uptake รักษา สูง ต่ำมาก GRAVES’ Low normal Transient painless thyroiditis Thyroiditis (probably Hashimato’s รักษา ติดตามอาการ + - blocker • .
Thyroid Nodule solitary multinodular FNAB TFT cystic solid or mixed hyperthyroidism Euthyroid Surgery or I131 FNAB malignant neoplasm follicular benign benign inadequate repeat FNAB US-FNAB malignant suspicious benign -L-T4 -observe scan+TSH benign Warm/cold hot surgery Symptom compatible winh malig- nant surgery No symptom reaspirate L-T4? Hyperthyroid (old patient, nodule>2.5 cm.) euthyroid (young patient, nodule<2.5 cm.) L-T4 or observe Surgery of I131 Rx Observe/follow up