Download
1 / 23
350 likes | 686 Views
Mineralization of Teeth. Damion Francis MSc. TMRI-ERU. Minerals. Chemical elements required by living organisms other than C, H, O, N Naturally occurring in foods and must be taken in the diet Comprise of 4% of the body weight Classified according to the amount needed by the body. Minerals.

E N D
Mineralization of Teeth Damion Francis MSc. TMRI-ERU
Minerals • Chemical elements required by living organisms other than C, H, O, N • Naturally occurring in foods and must be taken in the diet • Comprise of 4% of the body weight • Classified according to the amount needed by the body
Minerals • Macrominerals- required in large proportions by the body (≥100mg) • Includes: calcium, phosphorus, magnesium, etc. • Microminerals (Trace elements)- required in relatively small amount by the body • These include iron, zinc, cobalt and manganese
Mineralization of Bone and Teeth BONE • Bone is made up of an inorganic mass of minerals with a protein matrix (collagen) • Major component is calcium and phosphate along with a other minerals and trace minerals • Concurring with biological theory increase in fruit and vegetable intakes was associated with stronger bones in several studies
Mineralization of Bone and Teeth • The exchange of Ca and P between the extracellular matrix and body fluids are regulated by the parathyroid hormone (PTH) and vitamin D • Bone has two growth phases: • Formation of a protein matrix (collagen produced by osteoblasts) which can be calcified • Calcification (calcium phosphate is precipitated from serum)
Mineralization of Bone and Teeth • Remodeling involves the building of bone by osteoblasts which are then broken down by osteoclasts • Subsequently rebuilt by osteoblast mainly through the production of hydroxyapatite (Ca10(PO4)6OH2), the primary inorganic constituent of bone and teeth • The apatites develops and mature into calcified crystals increasing bone density
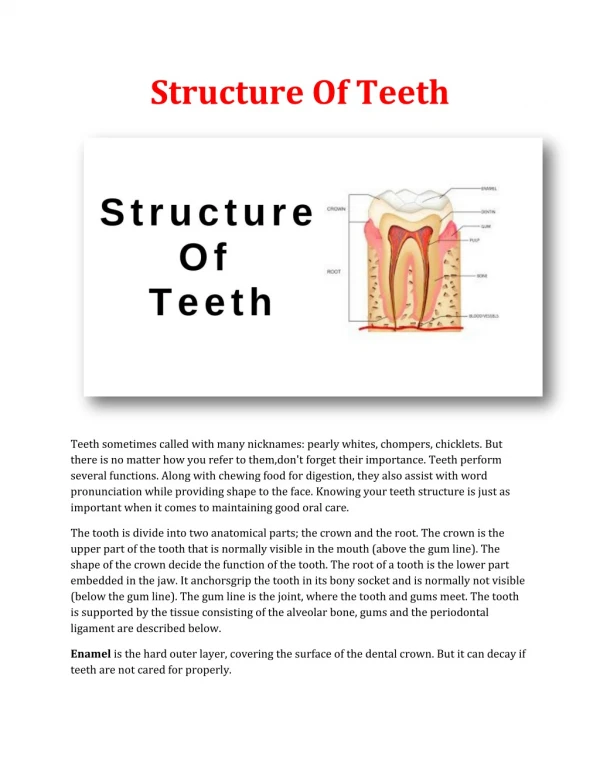
Mineralization of Bone and Teeth Teeth • Mineralization of cementum and dentin is similar to bone • Calcification of enamel differs from the above mentioned • Mineralization and matrix formation occur alongside enamel development • Mineral content of enamel is 95-97% with only a trace of organic matrix
Mineralization of Bone and Teeth • Enamel development begins with the differentiation of cells of the oral epithelium • Thickens to form a protruded inner enamel epithelium • Results in formation of ameloblasts which secretes enamel proteins such as amelogenin • Also involved in transport of calcium and phosphate in enamel matrix
Mineralization of Bone and Teeth • Enamel proteins such as amelogenin mediate the formation of hydroxyapatite crystals from calcium and phosphate through enamel biomineralization • Protein fraction in developing enamel is an aggregate of small proteins most of which are phosphoproteins • Once enamel is completely mineralized only phosphopeptides remain (phosphorus and 1 or 2 aa)
Calcium • Adult body contains 1-1.5kg of ca • Function • Deposit in soft tissue to harden them • Plays part in controlling heart action, skeletal muscle & excitability of the nerve • Has role in blood clotting (prothrombin & thrombin) • Enzyme cofactor (pancreatic lipase) • Chromosomal movement before meiosis
Calcium • Metabolism • Absorbed mainly in upper small intestine • Facilitatedby vit. D, proteins, acid pH • Reduced by phytic acid, oxalic acid • Transported as free ion or bound to albumin
Metabolism of Calcium • Blood levels are regulated by PTH, calcitonin (thyroid gland), and active vit. D • storage deposit of calcium is bone trabuculae in long bones • Bones are metabolically active but can calcium can be withdrawn when needed
Metabolism of Calcium • Approximately 250 – 1000mg of calcium enters and leave the bone daily • Homeostasis is maintained from dynamism between blood levels and bone • Diet and resorption contributes to the blood levels which act as a reserve • Osteoid formation is directly regulated by amount of calcium from diet
Calcium Balance • Calcium balance is obtained when there is sufficient calcium absorbed to meet body requirements for growth and tissue regeneration • Negative balance when insufficient consumed and body mobilize calcium from bone to maintain necessary blood levels
CALCIUM HOMEOSTASIS THREE HORMONE AND THREE ORGANS • PTH • ACTIVATED VITAMIN D • CALCITONIN • BONE • KIDNEY • SMALL INTESTINE
PTH • principal regulator of [Ca] in ECF by [Ca] and [Pi] • If blood levels of iCa 0.1 mg/dl, secretion of PTH is • Kidney reacts quickly to changes in PTH minute to minute adjustments of blood Ca • PTH acts on distal nephron to urinary excretion of Ca
Vitamin D • steroid hormone • regulate specific gene expression following interaction with its intracellular receptor • biologically active form is 1,25-dihydroxy vitamin D3 (1,25-(OH)2D3, also termed calcitriol) • calcitriol functions primarily to regulate calcium and phosphorous homeostasis
Calcitonin (32 amino acid ) • Parafollicular cells of thyroid gland in response of hypercalcaemia • Decrease osteoclast activity • Stimulating a distal tubular - mediated calciuresis Other hormones affect Ca balance - including prostaglandins that mobilize Ca, various growth factors, growth hormone, somatomedins, thyroid hormones (decrease skeletal mass), sex steroids which help maintain bone mass, adrenal cortical hormones
Calcium • Sources dairy product, fortified flour, egg,leafy vegetable, fish, cabbage, broccoli • Requirement Adult 500mg/day, Pregnancy 1200mg/day excreted in urine and feces • Deficiency Rickets in children & Osteomalacia in adult
Food Calcium Small Intestine Feces Unabsorbed calcium Alkaline pH Oxalic acid Phytic Acid Some Fibers Laxatives Body need Acid pH Vitamin C Vitamin D Lactose Certain amino acids Blood Calcitonin (thyroid hormone) Sufficient Vitamin D Weight-bearing exercise Parathyroid hormone Inadequate/ excess vit. D Bone immobilization Teeth Urine Bones Positive calcium balance Negative calcium balance
Oral Implications of Inadequate Calcium Intake • Inadequate intake, impaired absorption and increased loss include: • Incomplete calcification of teeth • Tooth and bone malformations • Increased susceptibility to dental caries • Excessive periodontal bone resorption • Increased tooth mobility and premature tooth loss • Increased risk of hemorrhage
Oral Implications of Inadequate Calcium Intake • Less than 500mg calcium associated with higher risk of gingival detachment • Decreased bone mineral density (cementum and dentin)