Download
1 / 1
10 likes | 82 Views
Do PNES Risk Factors That Discriminate for Diagnosis Predict Clinical Outcome? Caris, E; Took, L; Tracy, J; Nei, M; Skidmore, C; Mintzer, S; Zangaladze, A; Sperling, M; Glosser, D. . Department of Neurology, Jefferson Medical College, Philadelphia, PA, USA david.glosser@jefferson.edu.

E N D
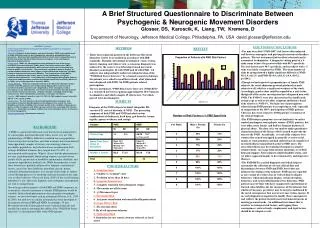
Do PNES Risk Factors That Discriminate for Diagnosis Predict Clinical Outcome? Caris, E; Took, L; Tracy, J; Nei, M; Skidmore, C; Mintzer, S; Zangaladze, A; Sperling, M; Glosser, D  Department of Neurology, Jefferson Medical College, Philadelphia, PA, USA david.glosser@jefferson.edu METHODS • Sixty one of 68 sequential admissions to the Epilepsy Care Unit were successfully followed up at an average of 9.8 months post discharge for the PNES patients and 11.7 months for the ES (epilepsy only) patients. Through clinical exam, history, imaging, and video-EEG, a consensus diagnosis was achieved in 64 of the admissions; 30 with PNES and 32 with ES. Two subjects with both ES and PNES were excluded. All patients underwent neuropsychological testing, administration of the “PNES-15 Risk Factor Structured Interview”, and a structured interview to determine health care utilization, employment, and estimated seizure frequency. • Each subject had a discharge conference with the attending neurologist to review the EEG findings, diagnosis, and follow-up recommendations arising from the hospitalization. Enrolled subjects all consented to a follow-up telephone interview; at which time a structured interview was conducted to collect data about seizure outcome, AED use, satisfaction with care, memory of discharge diagnosis, agreement with diagnosis, and interim healthcare utilization. A brief QOL. measure, “Satisfaction With Life Scale” (Deiner, et al., 1985), was administered as well. SUBJECTS Outcome Comparison of Higher vs. Lower # of PNES Risks in PNES Group PNES-15 RISK FACTORS Morphology/Semiology: ETOH History: 1. > 3 seizure types 12. > 12 drinks/wk, ETOH arrest 2. Pre-ictal headache family/MD complaints 3. Ictal eye closure Drug Abuse: 4. Ictal crying 13. Any IV, Rx NA dependence, 5. AED’s no help or worsen major drugs non-IV, family/MD seizures. Complaints 6. > 5 min. seizure duration Other Abnormal Illness Behavior: Mental Health Tx History: 14. Fibromyalgia, TMJ, RSD, 7. Prior psych consultation chronic pain syndrome, titer(-)Lyme Violence/Abuse functional Neuro or NP exam 8. SIB history Medico legal/Legal: 9. Suicide attempt 15. Injury, WC, malpractice suits, 10. Physical abuse history lawyer referred, arrest history 11. Sexual abuse history RESULTS ABSTRACT (revised) • Do PNES Risk Factors That Discriminate For Diagnosis Predict Clinical Outcome? • Rationale: Psychogenic non-epileptic seizures (PNES) are common and heterogeneous. Though diagnosis and treatment of PNES have become more sophisticated, and risk factors have been identified to differentiate between epilepsy and PNES, little work has been done to predict clinical outcome of PNES patients. We attempted to prospectively identify type and number of risks predictive of post-diagnosis outcome. • Methods: Sixty-eight sequential random admits to the Jefferson Epilepsy Care Unit were enrolled under IRB approval. Diagnosis was by history, exam, imaging, and video-EEG of typical seizures and inter-ictal periods. All S’s underwent neuropsych tests and the “PNES Risk Factor Structured Interview” assessing seizure semiology, psycho-social risks, and “abnormal illness behaviors”. Thirty patients were discharged with PNES diagnosis and 32 with epileptic seizures only (ES). Six subjects were excluded; 4 with uncertain diagnosis, and 2 with both ES and PNES. Follow-up failed with 4 PNES and 2 ES subjects. Gender, age, and IQ of the remaining 25 PNES (7 male) and 26 ES (6 male) S’s were equivalent. At mean discharge month 11.7 (ES) and 9.8 (PNES) a structured telephone interview of outcome variables including: medical utilization, quality of life (QOL), seizure frequency, and employment status was administered. The PNES subjects were further divided into two groups; a “lower risk” group with <7 total PNES risks (N=7; M=4.44, SD=1.42) and a “high risk” group with >7 risks (N=16; M=8.5, SD=1.37). • Results: PNES S’s endorsed a significantly greater number of risk factors than epilepsy S’s (M=7.04, SD=2.41 vs. M=3.31, SD=2; p<.001. Post-discharge, PNES S’s consulted more doctors (M=2.24, SD=1.96 vs. M=.62, SD=.98, p<.001) than ES S’s. PNES S’s also had lower scores on a 35 point QOL scale (M=19.4, SD=7.9 vs. M=25.7, SD=8, p=.006). At follow-up, S’s in the high and low risk groups did not differ significantly in number of reported seizures in last 30 days (M=8.06, SD=24.6 vs. M=18.1, SD=49.5), doctors seen (M=2.19, SD=1.68 vs. M=2.33, SD=2.5), emergency department visits (M=.44, SD=.63 vs. M=.22, SD=.67), current AEDs (M=.44 for both groups, SD=.63 vs. .53), months working full time (M=.75, SD=1.34 vs. M=1.78, SD=2.95, or QOL scores (M=17.9, SD=7.5 vs. M=22.1, SD=8.3). Finally, the total number of PNES risks was uncorrelated with any outcome variables. • Conclusions: The diagnosis of PNES was well predicted by a higher number of risk factors, and PNES patients demonstrated worse outcome in measured domains than even the often severely ill epilepsy patients admitted for monitoring. However, a higher number of risks did not predict worse outcome. Personal, historical, and semiological PNES risk factors may be regarded as vulnerabilities for the emergence of the abnormal illness behavior constituting PNES, but once the behavior emerges, its persistence may be determined by patterns of social response to it more than by the vulnerabilities which originally motivated it. This study is weakened by its reliance on patients’ subjective reports of seizure frequency and other variables; both at time of initial assessment and follow-up. DISCUSSION/CONCLUSIONS • The “PNES-15” risk factors discriminated well between epilepsy and psychogenic non-epileptic seizure patients; both male and female. The test instrument had excellent sensitivity and selectivity and is economical to administer. A diagnostic cutting point of > 3 for males and > 4 for women seems to have the greatest utility. • The PNES group had worse clinical status both at time of diagnosis and at 9-11 month follow-up than the ES patients, and the PNES group showed some clinical improvement at follow-up; reported elsewhere (Glosser, et al., 2008). However, in this relatively small sample, PNES patients with a higher number of risks did not fare worse at follow-up than the lower risk-number group. Among the PNES patients, none of the outcome variables correlated significantly with the number of risks. • Examination of the data reveals tremendous variance among the PNES groups’ self-reports of seizure frequency, number of doctors seen, and number of ER visits. When the PNES group is divided into “high” vs. “low” risk factor loading groups, the number of S’s becomes too low to register significance or to tolerate exclusion of outliers. Moreover, very few of the members of this PNES group had a truly “low” number of risks. Ideally, those with 3-5 risks should have been compared to a like number of those with 8-10 risks, but there were few with less than 7 PNES risks. Subsequently, a larger sample has been completed, and a logistic regression re-analysis of the data might yield more specific information about which combinations of risks predict outcome. • Finally, while various PNES risk factors may be regarded as constitutional or learned vulnerabilities for the emergence of the behavior, its persistence may be largely conditioned by the social consequences that accrue to it once it does emerge. An instrument sensitive to a different set of risk factors, tapping those consequences; such as family, employment, and legal factors should be developed. BACKGROUND Psychogenic non-epileptic seizures (PNES) are thought to occur in up to 30% of patients with intractable seizures and occasion lower quality of life, greater risk of morbidity and mortality, disability, and expensive unproductive medical care. A PNES is a paroxysmal behavioral event that has been medically interpreted to be an epileptic seizure when in fact it is a diagnostic misattribution which has the social effect of relabeling a behavior as a disease. What makes PNES behavior distinctive is that once it has been relabeled as epilepsy, potent culturally determined responses to it emerge which shape its further course. While the propensity to emit these behaviors is probably influenced by inherent constitutional factors and trauma, it has been argued that PNES is learned and modified through processes of modeling, reinforcement and extinction in the same way as other behaviors (Sirven & Glosser, 1998). If the social learning hypothesis is true, then early diagnosis and contingency management are vital to mitigate harm. An economical, sensitive, and selective instrument to identify PNES patients and predict outcome would be valuable. The “PNES-15 Risk Factor Structured Interview”, developed at the Jefferson Epilepsy Center (Glosser, et al., 2003), reliably discriminates between PNES and epilepsy patients, but until now, no study has been undertaken to determine if the number or type of risk factors predicts clinical outcome. Accordingly, 68 sequential admissions to the Epilepsy Care Unit were monitored and followed up after discharge to determine the ability of the “PNES-15” to discriminate PNES From epilepsy (ES) patients and to determine if type and number of risk factors predict outcome of the PNES patients.