Download
1 / 1
10 likes | 110 Views
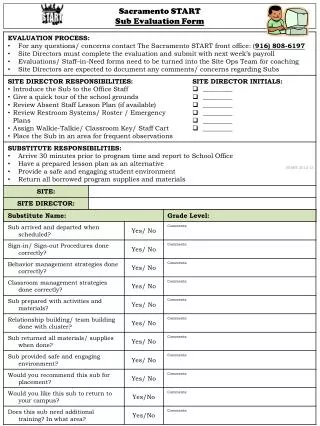
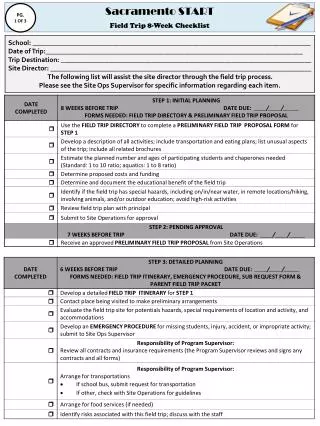
Sacramento START Time-Off Notification . TIME-OFF REQUEST FORM NAME: ________________________________________ EMAIL ADDRESS : ________________________________________ SITE : ________________________________________

E N D
Sacramento STARTTime-Off Notification TIME-OFF REQUEST FORM NAME: ________________________________________ EMAIL ADDRESS:________________________________________ SITE: ________________________________________ POSITION: _______________________________________ CONTACT NUMBER: _______________________________________ REASON FOR REQUEST: ________________________________________ REQUESTED DATES: ________________________________________ Request Steps: Field Staff Staff Member Request – complete the time off request form & submit for approval Site Director Authorization – complete approval section for time off request & submit with payroll Sub Coordinator Authorization – complete approval for Sub Request & contact sub staff Program Supervisor Authorization – complete approval for time off request & provide copy for site staff Be Advised: All Requests must be submitted 2 weeks in advance, including Mandatory Trainings! AUTHORIZATION SITE DIRECTOR: X__________________________________ APPROVAL: _____Yes _____ No Date: __________ COMMENTS: __________________________________________________________________ SUBSTITUTE COORDINATOR: X__________________________________ SUB ASSIGNED: _____Yes _____ No Date: __________ COMMENTS: __________________________________________________________________ PROGRAM SUPERVISOR: X__________________________________ APPROVAL: _____Yes _____ No Date: __________ COMMENTS: __________________________________________________________________ 2013-14