Download
1 / 47
480 likes | 714 Views
Osteoporosis. Emily Webb, M.D. Overview. Pathophysiology Prevention Screening Secondary causes Medications. Bone Types. Cortical- outer shell of bones Trabecular- spongy, internal support. Bone Strength. Density Turnover Size Shape Microarchitecture Damage accumulation

E N D
Osteoporosis Emily Webb, M.D.
Overview • Pathophysiology • Prevention • Screening • Secondary causes • Medications
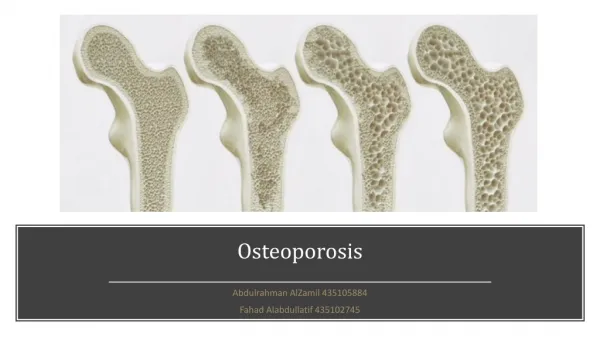
Bone Types • Cortical- outer shell of bones • Trabecular- spongy, internal support
Bone Strength • Density • Turnover • Size • Shape • Microarchitecture • Damage accumulation • Mineralization • Matrix quality
Remodeling Cycle • Resting • Resorption • Reversal • Formation
Calcium • 98% stored in bones • Regulated by intestinal, renal, and skeletal systems • If inadequate dietary supply of calcium, will reabsorb skeletal stores to maintain plasma levels.
Vitamin D • 95% of vitamin D is from sunlight • Vit D 25(OH)D 1,25(OH)2D • Increases GI calcium absorption • Measure 25(OH)D to determine deficiency
Vitamin D deficiency • Vit D deficiency secondary hyperparathyroidism (SH) mobilize bone calcium stores normal serum calcium • SH decreases phosphorus levels inadequate to mineralize skeleton • Kids = rickets • Adults = osteomalacia
Parathyroid Hormone • Increases renal calcium reabsorption • Stimulates renal vitamin D production • Releases calcium from the bone
Osteoclast Activity • Vitamin D deficiency • Estrogen deficiency • Parathyroid hormone excess • Hyperthyroidism
Bone Loss • Bone mass peaks at age 30 • Then 0.4 % bone lost per year • First 5-8 years after menopause, women lose 2% of cortical and 5% of trabecular bone per year • Early menopause- increased osteoclasts • Later menopause- decreased osteoblasts
Modifiable Risk Factors • Smoking • Alcoholism • Inadequate physical activity • Long-term low calcium or vitamin D intake • Poor nutrition
Potentially Modifiable Risk Factors • Estrogen deficiency • Low weight/BMI (<127 pounds) • Recurrent falls • Chronic steroid use • Thyroid hormone • Anticonvulsants
Hx of fracture FHx- first degree relative Caucasian/Asian Dementia Age Fraility Impaired eyesight Non-Modifiable Risk Factors
Amyloidosis Ankylosing spondylitis COPD Congenital porphyria Cushing’s disease Eating disorders Female athlete triad Gastrectomy Gaucher’s disease Hemochromatosis Hemophilia HIV Hyperparathyroidism Hypogonadism Hypophosphatasia Idiopathic scoliosis Inflammatory bowel IDDM Lymphoma & leukemia Malabsorption syndromes Mastocytosis Multiple myeloma Multiple sclerosis Pernicious anemia Medical Conditions
Medical Conditions • Rheumatoid arthritis • Severe liver disease • Spinal cord transsection • Sprue • Stroke • Thalassemia • Thyrotoxicosis
Aluminum Anticonvulsants Cytotoxic drugs Glucocorticosteroids GnRH agonists Immunosuppressants Lithium Long-term heparin Progesterone, parenteral, long acting Supraphysiologic thyroxine doses Tamoxifen (premeno) TPN Drugs Associated with Osteoporosis
Prevention of Fractures • Weight bearing exercise • Prevent falls • Limit sedating medications • No smoking • Limit alcohol • Calcium (800 mg 4-8 yo, 1300 mg 9-18 yo) and vitamin D (400-800 IU daily) • Some sunlight
Daily Elemental Calcium • Premenopausal women 25-50 years old: 1,000 mg • Postmenopausal women less than 65 years old on estrogen: 1,000 mg • Postmenopausal women not on estrogen: 1,500 mg • All women older than 65 years: 1,500 mg
Institute of Medicine • Young adults: 1,000 mg daily • 50 years old and older: 1,200 mg daily
Dietary sources of calcium • Milk 8 ounces = 300 mg • Yogurt 8 ounces = 400 mg • Cheese 1 ounce = 200 mg • Fortified foods and juices
Vitamin D • Fish, egg yolks, fortified milk • <50 yo- 200 IU • 50-70 yo- 400 IU • >70 yo- 600 IU • If minimal sun exposure, 1000 IU
Screening • Women aged 65 and over • Men aged 70 and over • Every two years unless a new risk factor develops • Postmenopausal with 1+ risk factors • All postmenopausal women with a fracture • Chronic steroid use
DXA • Dual energy x-ray absorptiometry • Lumbar spine and hip • Use the same machine • T score- SD above/below the mean for young adults of the same sex • Z score- compared with reference population of the same age, race, sex • For every standard deviation decrease, risk of fracture doubles
Secondary Causes • Hypogonadism • Hyperparathyroidism • Rheumatologic disorders • Malignancy • GI disorders • Vitamin D deficiency • Chronic steroid use
Workup for Secondary Causes • First: serum calcium, serum chemistry, 24 hour urine calcium and creatinine, parathyroid hormone, TSH if taking thyroid hormone • Second: renal profile, vitamin D level, thyroid function, serum protein electrophoresis, maybe cortisol level if worried about Cushings
Cost Effective Work-Up • For $75 per patient (85%): 24 hour urine calcium, serum calcium, serum PTH • For $116 per patient (98%): add vitamin D
When to Treat • T score –2 without risk factors • T score –1.5 with risk factors • Z score –1 (look for secondary causes)
Bisphosphanates • Alendronate (Fosamax) and risendronate (Actonel) • Inhibit osteoclasts • Decrease fractures (spine and nonvertebral) in osteoporosis • Prevention and treatment • Upper GI side effects • Poor absorption <1% • Take on an empty stomach with water, upright for 30 min without food or drink, weekly or daily
Bisphosphanates Studies • Fracture Intervention Trial • Vertebral Efficacy with Risendronate Therapy in North America • Fosamax Actonel Comparison Trial
SERMs • Estrogen like effects on the skeleton • Raloxifen • Tibolone • Tamoxifen
Raloxifen (SERM) • Binds to estrogen receptors on bone to decrease bone resorption and increase BMD • Prevention and treatment • Decreases vertebral fx in women with osteoporosis, but no reduction in hip fx • No endometrial stimulation • Possible decrease in breast cancer • Side effects- vasomotor, clots • Risks similar to estrogen
Tibolone • Androgen and progesterone effects • Prevention of bone loss • Still in trials
Tamoxifen • Chemoprevention for breast cancer • Slight decrease in bone fracture risks • Side effects- vasomotor, stimulates endometrium
Hormones • Inhibits osteoclasts • FDA approved for prevention of osteoporosis • Since WHI, not first line • Prempro • Menostar (estradiol transdermal)- weekly
Salmon Calcitonin • Nasal or subcutaneous • Treatment, not prevention • Inhibits osteoclasts • Approved for women who are 5 years postmenopause • Works for spine, but not hip fractures • Decreases bone pain from vertebral fx • Side effects- nausea, flushing
Teriparatide • Fragment of parathyroid hormone • Subcutaneous daily • Increases trabecular bone density and connectivity • Postmenopausal women • Treatment, not prevention • Use when other treatments fail • Expensive • Don’t use in combination with the bisphosphonates
Prevention • Bisphosphonates • Raloxifene • Estrogen
Treatment • Bisphosphonates • Raloxifene • Calcitonin • Parathyroid hormone
Repeat DXA • Every 3-5 years in untreated postmenopausal women (T > -1) • Every 2 years in treated women • Yearly if on steroids or elevated PTH • Every 1-2 years if osteopenia • Spine shows improvement earlier than hip
New Technology • MRI for microarchitecture and cross-section geometry • CT for cross-section geometry • Ultrasound of heel may predict hip fracture • Research only
Conclusion • Prevention • Screening • Treatment
References • Bilezikian, Holick, et al. “Osteoporosis: Diagnosis, Treatment, and Monitoring Considerations.” CME Forum. Vol. 3 Boston University School of Medicine. March 2004. • Mechcatie, E. “Secondary Causes of Bone Loss Often Missed.” Ob.Gyn. News. March 2003. • Osteoporosis Insight 2004. University of Texas Southwestern. Jersey City, NJ. Vol. 1. • “Osteoporosis.” ACOG Practice Bulletin. January 2004. Pg 203-216.
References • Sullivan, M. “Teens Lose Bone on DMPA, Recover It After Stopping Use.” Ob.Gyn. News. March 2003. • The 2004 Surgeon General's Report on Bone Health and Osteoporosis: What It Means To You