Download
1 / 36
360 likes | 379 Views
Osteoporosis. an underestimated disease. Definition of osteoporosis. …a systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue leading to enhanced bone fragility and a consequent increase in fracture risk.

E N D
Osteoporosis an underestimated disease
Definition of osteoporosis …a systemic skeletal disease characterized by low bone mass and microarchitectural deterioration of bone tissue leading to enhanced bone fragility and a consequent increase in fracture risk. World Health Organization (WHO). Technical Report Series 843, Geneva 1994Update TRS 921, 2003
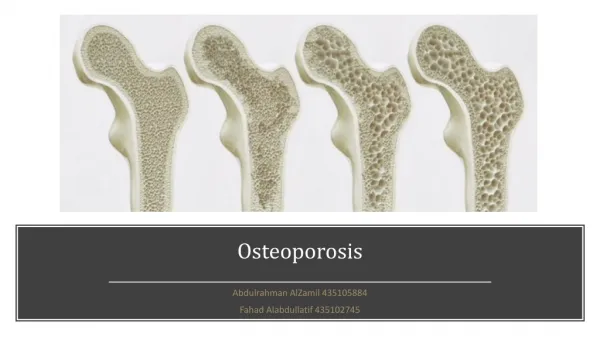
normal osteoporotic
Osteoporosis diagnosis Areal bone mineral density is a important predictor of fracture risk. Spine/hip dual energy X-ray absorptiometry measurement (DEXA) is the diagnostic standard WHO. Technical Report Series 921, Geneva 2003
Dual Energy X-ray Absorptiometry or DEXA • Measures X-ray absorption • Bone mass per projected area (g/cm2) • BMD correlates with whole bone strength Bouxsein ML, et al. Bone 1999; 25(1):49-54.
BMD T-score=number of SD vs. mean BMD of healthy young female population (at peak bone mass) WHO, 1994 – update 2003
DEXA as BMD-measurement method Peak Bone Mass Osteoporosis Normal Osteopenia 0 –1 –2 –2.5 T-score DEXA = Dual-Energy X-ray Absorptiometry
‘Established osteoporosis’ WHO criteria for osteoporosis in women World Health Organization (WHO). Technical Report Series 843, Geneva 1994Update TRS 921, 2003
Diagnosis of Osteoporosis • BMD T-score -2.5 DEXA and / or • presence (history) of osteoporotic fracture RX
Osteoblast Osteoclast imbalance of bone-remodeling Age 40 Age 60 Age 70 Progression of vertebralfractures in osteoporosis
1989 1996 1959 Inger Lundegaardh, Sweden IOF: international osteoporosis foundation, http://www.osteofound.org
Pathophysiology of osteoporosis:bone remodelling Lining cells cover resting bone Osteoclasts resorb bone Activation resorption phase ~20 days Bone Bone Osteoblasts lay new osteoid Reversal formation phase ~160 days Bone Bone Newly laid osteoid mineralises overseveral months
Postmenopausal bone loss: role of estrogen deficiency Indirect effects Estrogen deficiency Dietary calcium(decreased absorptiondue to Vit. D deficiency) ? Directly increasesosteoclast number and longevity Decreased bone formation Secondary hyperparathyroidism Increased bone resorption Remodelling imbalance Bone Loss Adapted from Riggs BL, et al. J Bone Miner Res 1998; 13(5):763-773.
Age-related bone lossoccurs in men and women I Men I III Women II Bone mass III I Peak bone mass II Rapid bone loss (menopause)III Age-related bone loss 0 20 40 60 80 100 Age (years)
Bone Remodelling throughout Life Bone turnover = a coupled process always : bone resorption → bone formation • Childhood & adolescence: resorption < formation • As from the age of 40: resorption > formation • always negative balance per bone remodelling cycle • slow bone loss • Postmenopausal period: accelerated bone loss • estrogens inhibit bone turnover • E-deficiency → higher bone turnover rate
Low TURNOVER = low BONE LOSS High TURNOVER = high BONE LOSS Pathogenesis of Osteoporosis > 40 y negative net balance per bone remodelling cycle
Distribution of trabecular and cortical bone throughout the skeletal system Femoral neck25% trabecular75% cortical Vertebrae66% trabecular34% cortical Forearm(distal radius)20% trabecular80% cortical Trochanteric region50% trabecular50% cortical adapted from http://www.merckmedicus.com
Incidence of osteoporotic fractures in women Vertebrae Annual incidence Hip Wrist 50 60 70 80 Age (years) Adapted fromWasnich RD, Osteoporos Int 1997;7 Suppl 3:68-72and Sambrook P et al. Lancet 2006; 367(9527):2010-2018
Lifetime fracture risk of people at 50 years of age Adapted from Melton LJ, III, et al. J Bone Miner Res 1992; 7(9):1005-1010. .
All fractures are associated with morbidity One year after a hip fracture Unable to carry out at least one independent activity of daily living 80% Patients (%) Unable to walk independently Discharged toNursing Home 40% Death within one year 30% ≥20% Adapted from Cooper C. Am J Med 1997; 103(2A):12S-17S.
Morbidity after vertebral fractures • Back pain • Loss of height • Deformity (kyphosis, protuberant abdomen) • Reduced pulmonary function • Diminished quality of life: loss of self-esteem, distorted body image, dependence on narcotic analgesics, sleep disorder, depression, loss of autonomy, social dependence • Increased mortality http://www.osteofound.org/
Age-Standardized Mortality Ratio FractureWomen Men Proximal femur 2.2 3.2 Vertebral 1.7 2.4 Other major 1.9 2.2 Minor 0.8 1.5 Mortality after major types of osteoporotic fracture in men and women 5 - Year Prospective Cohort Study Adapted from Center JR, et al. Lancet 1999; 353(9156):878-882..
Economic Impact Number of bed days (men and women)in Switzerland in 1992: 701,000 for osteoporosis 889,000 for chronic obstructive pulmonary disease 533,000 for stroke 328,000 for myocardial infarction 201,000 for breast cancer Osteoporosis # 1 when looking at women only Adapted fromLippuner K, et al. Osteoporos Int 1997; 7(5):414-425.
Risk factors that provide indications for the diagnostic use of bone densitometry • Presence of strong risk factors • Previous fragility fracture • Radiographic evidence of osteopenia or vertebral deformity or both • Loss of height, thoracic kyphosis(after radiographic confirmation of vertebral deformities) Kanis JA. Lancet 2002; 359(9321):1929-1936.
Risk Factors that identify people who should be assessed* for Osteoporosis Minor Risk Factor Major Risk Factors • Age 65 years • Vertebral compression fracture • Fragility fracture after age 40 • Family history of osteoporotic fracture(esp. maternal hip fract.) • Systemic glucocorticoids (> 3 m) • Early menopause (before 45) • Malabsorption syndrome • Primary hyperparathyroidism • Propensity to fall • Osteopenia apparent on x-ray film • Hypogonadism • High Bone Turnover • Major immobility • Rheumatoid Arthritis • Hyperthyroidism • Anticonvulsant therapy • Chronic heparin therapy (UFH) • Calcium Intake < 500 mg/d • Smoking • Excessive alcohol intake • BMI < 19 * BMD measurement is recommended for those with at least 1 major or 2 minor risk factors . Adapted from Brown JP, et al. CMAJ 2002; 167(10 Suppl):S1-34.
Who to test (BMD-measurement) for Postmenopausal Osteoporosis ? • post-menopausal, 65 y • post-menopausal, < 65 y • with additional risk factors, or • with fragility fracture, or • with loss of height or deformity of the spine (kyphosis) • pre- or post-menopausal • with disease or receiving a treatment, known that they can cause a ‘secondary’ form of osteoporosis Adapted from Raisz LG. N Engl J Med 2005; 353(2):164-171.
Preventing osteoporosis C alcium D Vitamin E xercise F Prevent alls G ain weight S Stop moking
TREATMENT of OSTEOPOROSISin order to prevent (new) fractures
Strontium ranelate Drugs used in osteoporosis treatment • HRT • SERM/Raloxifene • Calcitonin • Bisphosphonates-Alendronate- Risedronate- Ibandronate • Parathyroid hormone Inhibition of resorption Stimulation of formation