Download
1 / 93
930 likes | 931 Views
Explore evidence-based practices for individuals with Autism Spectrum Disorder and co-occurring conditions, including ADHD, anxiety, depression, and psychosis.

E N D
Evidence-Based Interventions for Autism Spectrum Disorder and Co-occurring Diagnoses Deidre Donaldson, PhD, ABPP, LABA, BCBA May Institute and the National Autism Center
ASD and Mental Health • Introduction • Brief overview of ASD • Co-occurring conditions • Evidence-based practices • Q&A
Services for Autism spectrum disorders Assessment and Diagnosis Educational Services (5 private schools) Adult Day and Residential Services Home- and Clinic-based ABA services Family Support Services, Groups International Consultation
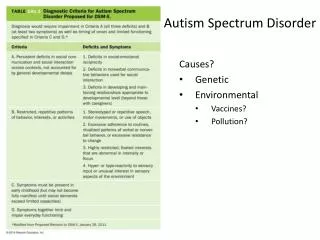
Autism spectrum disorder(DSM-5)Core deficits • Persistent deficits in communication and social interaction across multiple contexts • Restricted, repetitive patterns of behavior, interests, activities
Autism spectrum disorder(DSM-5) • Appears early in development • Causes clinically significant impairment in important areas of daily functioning • Not better accounted for by I/DD or global developmental delay
Autism spectrum disorder(DSM-5) Specifiers: • Intellectual impairment • Language impairment • Medical or genetic factors • Catatonia
Autism spectrum disorder(DSM-5) Differential diagnoses: • I/DD without ASD • Social communication disorder • Rhett syndrome • Selective mutism • Schizophrenia
Autism spectrum disorder How is life affected? • Social relationships • Adaptive skills • Learning • Family
Autism spectrum disorder • Parenting stress • "Need Assistance" (Strunk, Pickler, McCain, Ameringer, & Myers, 2014): • Medication management • Navigating healthcare • Secondary health problems • Need for resources & services like Respite, Finances
Autism spectrum disorder https://www.youtube.com/watch?v=minoNnY-Izk
Autism spectrum disorder If you've met one individual with autism, you've met one individual with autism -Brenda Smith Myles
Autism spectrum disorder Issues in diagnosis: • Increasing rates • Evidence-based assessment • Age at presentation • Cultural differences • Co-occurrence with other disorders
Autism and mental health • Co-occurrence recognized in psychiatry for over 30 years • Core deficits increase risk for psychiatric disorder and psychiatric comorbidity compounds the problems of core deficits • 70% of individuals with ASD have 1, 40% for 2 (DSM-5, 2015) • Co-occurrence of ASD with another MH disorder is 2x as likely as those with I/DD as ASD without I/DD
Autism and mental health • ADHD • Anxiety (including OCD) • Borderline Personality Disorder • Depression/Mood (including Bipolar Dx) • Psychosis • Substance Abuse
Autism and mental health What co-occurring problems do you observe? (on-line poll)
https://www.polleverywhere.com/multiple_choice_polls/T8yX7GEZMUSasrohttps://www.polleverywhere.com/multiple_choice_polls/T8yX7GEZMUSasrohttps://www.polleverywhere.com/multiple_choice_polls/T8yX7GEZMUSasrohttps://www.polleverywhere.com/multiple_choice_polls/T8yX7GEZMUSasro
Autism and mental health Buck et al., 2014
Autism and health Medical comorbidities: • Gastrointestinal • Feeding • Pica • Sleep • Seizures
Autism and anxiety Significant Anxiety or Anxiety Disorder 40-56% of those with ASD • Phobias: 44% • Social Anxiety: 22-29% • GAD: 13-20% • Panic Dx: 10% • OCD 1-4% community samples >17% in ASD (e.g., Lugnegard, Hallerback, Gillberg, 2014; Steensel, Bogels, & Perrin, 2011)
Autism and ADHD ADHD: 30% (Lugnegard et al., 2011) • Slow processing speed • Increased impulsivity • Easily distracted • Severe difficulty shifting attention away from preferred activities, topics, etc. • Difficulty with transitions • Increased likelihood of externalizing behaviors (tantrums—yelling, name-calling, throwing/breaking things, self-injurious behaviors, repetitive behaviors).
Autism and substance abuse Substance Abuse: 0-11% Mostly in individuals with co-occurring ASD & ADHD (Lugnegard et al., 2011) • Obsess and perseverate on the effects of the substance • Untreated substance abuse—lack of training/specialization in ASD by providers • Criminal justice system
Autism and dEPRESSION Mood: 70% "Strikingly high" lifetime prevalence of MDD in young adults with ASD; m age =27 years) Unipolar depression: 10-25% in adolescence; 30-40% of ASD in adulthood Bipolar depression: More than unipolar, check family history, hypomania difficult to pick up • Social processing difficulties • Cognitive processing limitation (e.g., problem solving, coping) • Social isolation, poor social relationships • Oppositional, argumentative (Lugnegard, Hallerback, & Gillberg, 2014)
Autism and psychosis Psychosis: 2 - 20% • Misdiagnosis • Social isolation • Other people are fearful • Over-medicated • Poor medication and treatment adherence (Lugnegard et al., 2011; Hofvander, Delorme, Chaste, Nyden, et al., 2009)
psychosis Psychosis • Delusions--fixed false beliefs, out of keeping with cultural norms, and held against all evidence to the contrary (Kuperburg, 2010) • Hallucinations (auditory—voices; visual; olfactory; tactile; gustatory) • Disorganized thinking (speech) • Loose association, tangentiality, derailment, circumspect
Psychosis • Grossly disorganized or abnormal motor behavior (including catatonia) • Neologisms, non-words • Negative symptoms • lack of voluntary behavior or lack of motivation (avolition, amotivation) • apathy, flat or inappropriate affect • poverty of speech and language
Autism and psychosis Shared/overlap symptoms: • Unusual motor behavior • Repetitive movements (rocking, etc.) • Catatonia • Repetitive verbal behaviors (perseverative sounds, palilalia, echolalia) • Restricted range of affect/blunted affect • Poverty of thought or speech (inability to discuss or think about even a preferred topic at any level of depth or sophistication) • Paranoia/distrust of others, systems, government
Autism and psychosis Symptom overlap between ASD and Psychosis • A significant percentage of individuals diagnosed with an ASD as children lose that diagnosis by young adulthood and gain a diagnosis of schizophrenia/psychotic disorder. • The DSM-V allows co-diagnosis of a psychotic disorder (including schizophrenia) and an ASD. • The presentation of someone with an ASD and a psychotic disorder can be confusing
Autism and psychosis Case examples of delusions in individuals with ASD: • I have no bones in my body. • My skin is melting. • I have no organs in my body. • I have been reborn many times—first as an animal in prehistoric times, then as a Mayan girl who was kidnapped by Aztecs to be a slave. . . I was Ponce de Leon . . . I was Anne Frank. I am in love with Adolph Hitler.
Autism and psychosis Case example #1 of confusing presentation of individual with ASD and psychosis: “Hi, Joe.” (therapist) “You know the rooster.” (individual with ASD) “What rooster?” “The rooster. You know the rooster.” “Which rooster?” “The rooster. You know the rooster.” “I don’t know any rooster. Let’s go into my office and we can talk more.”“But you know the rooster, right? I know you know the rooster.”
Autism and psychosis “Nope. I’m sorry, but I don’t know what you’re talking about. You’ll have to explain once we get to my office.” “I know you know the rooster.” “Ok. Let’s go back now.” “You know the rooster.” Yells — “Don’t snuff the rooster!!...” In this interaction, the individual was not delusional or hallucinating, but was perseverating on a song.
Autism and psychosis Case example #2 of confusing presentation of individual with ASD and psychosis: “I was talking with Kurt today at school.” (individual with ASD) “Oh yeah? How is Kurt?” (therapist) “He was really mad.” “Why was he mad?” “Because of what the other kids did.” “What did the other kids do?” “He wanted me to say something, but I didn’t.”
Autism and psychosis “What did he want you to say?” “He was mad because I didn’t say it.”“Does he often tell you what to say?” “Yes. And if I don’t say it, bad things will happen. He will make them happen.” “What bad things?” “So he got mad at me.” “Does Kurt have other friends at school?” “He only visits me.” This young adult was describing auditory and visual hallucinations.
ASD & Psychosis—how to interact • Expect: the unexpected, to feel confused/manipulated/frustrated/worried. • Be calm • Be matter-of-fact with them about their behaviors and symptoms • Ask direct questions about their internal experiences • Are you hearing voices? • What are they saying? • Are you seeing things I can’t see? • What do you see? • Be accepting and non-judgmental of their answers • Just roll with it.
ASD & Psychosis—how to interact • Sympathize and empathize • Don’t directly contradict what they are saying. If the person is open to it, gently help him engage in reality testing by presenting other perspectives as possibilities • Acknowledge and confirm that the two of you are having different experiences. • Ask what has worked to help symptoms in the past
ASD & Psychosis—How to interact Response format • agreeably acknowledge what she said • explain why you asked • refer back to a previous conversation that went well and remind her what she said then • refer to a highly preferred topic • Try to get the person involved in an activity that interests her/him.
ASD & Psychosis—How to interact • Know the individual • Preferred topics and rewards • Be ready to replay a conversation that the person clearly enjoyed
Screening • Symptoms, behaviors • Identification of risk, triage • Follow-up on progress
EVIDENCE-BASED PRACTICES Clinical Expertise Individual Values and Preferences Best Research Evidence EBP Sackett, Straus, Richardson, Rosenberg, & Haynes, 2000
National Standards project • Comprehensive and Systematic Review of the literature of interventions for autism spectrum disorder • Educational and Behavioral interventions • Large, multi-year effort • Evidence-based practice guidelines • Phase 1 – 2009 • Phase 2 – 2015 (NSP-2)
National standards reports nationalautismcenter.org
National standards reports • www.mayinstitute.org • All U.S. states and 170 other countries • 340,000 unique visitors • 1.6 million page views • 115,000 downloads • 8,000 copies provided via grant funding
Selection of 27 expert panelists who have demonstrated expertise in the field of ASD. • These experts help select over 50 expert reviewers who coded research studies using a Scientific Merit Rating Scale (SMRS) to rate experimental rigor of the studies 0-5 Composite • Intervention Effects Rating Scale – Revised Beneficial, Ineffective, Unknown