Download
1 / 57
680 likes | 1.08k Views
Autism Spectrum Disorder. By Anna Jack, Ruth Jeffery, Kim McNaught & Stephanie Smith EDTE 620. AUTISM SPECTRUM DISORDER. 5 Disorders Diagnostic category of PERVASIVE DEVELOPMENTAL DISORDER (PDD) Childhood Disintegrative Disorder (CDD) Rett’s Disorder (RD) Autistic Disorder (AD)

E N D
Autism Spectrum Disorder By Anna Jack, Ruth Jeffery, Kim McNaught & Stephanie Smith EDTE 620
AUTISM SPECTRUM DISORDER • 5 Disorders • Diagnostic category of PERVASIVE DEVELOPMENTAL DISORDER (PDD) • Childhood Disintegrative Disorder (CDD) • Rett’s Disorder (RD) • Autistic Disorder (AD) • Pervasive Developmental Disorder – Not otherwise Specified (PDD-NOS) • Asperger’s Syndrome (AS)
AUSTISM DISORDER • Most common neurological disorder • 20 in 10,000 = 73,000 Canadians • One of the most common developmental disabilities affecting Canadians • Cognitive impairments • Deficits in verbal and non-verbal communication • Deficits in social understanding • Unusual behaviours, restricted activities
ASD’s change the way the brain processes information and can affect all aspects of a person’s development. • Classic autism usually manifests itself before the age of three years. • Boys have an incidence of 4 X that of girls.
AUTISM comes from the Greek word for SELF Describes the fact that the children seemed to lack interest in other people.
HISTORY • Dr. Leo Kanner in 1943 (psychiatrist) came up with term and classification of autism. • Based on observations of 11 child patients with similar behaviour. • Before this many would have been classified as emotionally disturbed or mentally retarded.
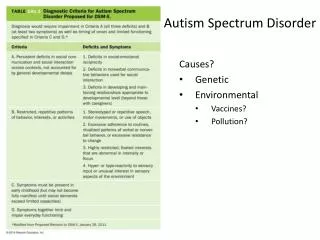
Proposed Causes • “Refrigerator Moms” which were educated working mothers that were cold and emotionally rejecting. • Caused by a disorder of language development which was dismissed since some autistics have good language skills. • Problems during birth • Genetics • Bowel and feeding problems leading to possibilities concerning the gastrointestinal tract. • Allergies and autoimmune disease. • Toxic and viral insults during fetal development • Drug Thalidomide carried a risk. • Mothers who had rubella during pregnancy had a higher risk • Viral infections • Thimerosal which is a form of mercury used in vaccines.
Today, most experts believe that autism is caused by a combination of genetics and an environmental factor.
SOCIAL INTERACTION • No interest in people at all or prefer to be left alone. May not notice when people are talking to them. “SELF” • Difficulty joining in. Cannot read or understand other people. Not know how to talk, play or relate to others. • May prefer company of adults. • Little or no eye contact. Use peripheral vision. • May not respond to or understand smiles or facial gestures. • Touch may feel painful or upsetting. May not cuddle or like to be held. May have their own terms. • Trouble talking about their own feelings or understanding other’s feelings. • Difficulty controlling emotion and excitement. Problem affects social interaction.
RESPONSES TO SENSATIONS • May have both auditory and visual processing problems and sensory input may be scrambled or overwhelm them. Varies from hypo to hyper sensitivity. • Unusual sensitivities to sounds, sights, touch, taste and smells. Ex. • fire alarm=painful • rough or scratchy fabrics may be intolerable • Sensitive to flickering flourescent lights Some may have very high pain thresholds or very low pain thresholds
VERBAL AND NON-VERBAL COMMUNICATION • Speech and language skills may begin to develop and then be lost, or may develop very slowly, or not at all. • 40% of children with ADS do not talk at all without intensive early intervention. • Communicate with gestures or pointing. • Difficulty with imitating sounds or words. • Some have echolalia (repeating something heard). May be repeated right away or much later and sometimes over and over. • Words used without usual meanings. Ex..He instead of she. • Non-verbal communications may not be understood such as waving good-bye. • Flat sounding voices with unusual pitch and rhythm. • Hard to initiate communication and to keep conversation going. Some speak very well but have a hard time listening to others.
REPEATED AND UNUSUAL BEHAVIOURS, INTERSTS AND ROUTINES • Ritualistic actions that are repeated over and over again. Ex. spinning, rocking, staring, finger flapping, etc. • Overactive or very passive • Can show intense anxiety or unusual lack of anxiety. • Unusual postures, walking or movement patterns • Very dependant on routines and things staying the same. No surprises. Ex. dressing in same order, going to school via new route, or new people around can trigger distress or fear. • Restricted pattern of interests. Obsessive about one things, idea, activity, or person. Sometimes these are unusual or socially inappropriate.
CO-OCCURRING CONDITIONS • Many with autism have other health problems: • Neurological disorders such as epilepsy • Gastro-intestinal problems • Compromised immune systems • Fine and gross motor deficits • Anxiety and depression
“POSSIBLE” Traits • Insistence of sameness • Difficulty in expressing needs • Repeating words or phrases • Laughing and/or crying for no apparent reason • Preference for being alone: aloof manner • Tantrums • Difficulty in mixing with others • Not wanting to cuddle or be cuddled • Little or no eye contact
Possible Traits Con’t • Unresponsive to normal teaching methods • Sustained odd play • Spinning objects • Obsessive attachment to objects • Apparent hyper or hypo sensitivity to pain • No real fear of danger • Noticeable physical over-activity or under-activity • Uneven gross/motor skills • Non-responsive to verbal cues, as if deaf
Many ASD individuals run contrary to many of the traits. • Some do make eye contact just not as frequently. • Some develop very good functional language or communication skills. • Some do take and give affection but usually on their own terms. • They do NOT however outgrow ASD.
UNIQUE ABILITIES • Some with ASD’s have an accurate and detailed memory for information and facts, high visual recall and ability to manipulate data for useful purposes. • May be able to concentrate for long periods of time on particular tasks or subjects. • Unusually good spatial perception and exceptional long-term memories which allows them to excel in areas such as: Music physics mechanics math science architecture
Learning Characteristics • Visual aids such as visual schedules to help with transitions. Helps to relieve stress if they know what is coming next. • Working in pairs which allows with social development. Making friends and developing relationships. Helps with integration. • Teacher’s aide to provide more detailed instructions. Helps student stay on same level as rest of class. Partial one-on-one lessons. • High levels of stress and anxiety. Working on Social Stories can reduce this. Teaching social and emotional concepts can help with controlling excessive behaviour reactions. • EACH CHILD WILL BE DIFFERENT. TEACHER NEEDS TO GET TO KNOW STUDENT TO LEARN WHAT THEY WILL NEED.
Helping Autistic Individuals • Applied Behavioural Analysis –ABA – oldest and most researched treatment. Reward based training focussing on teaching specific skills. • Speech Therapy • Occupational Therapy – fine motor skills and sensory integration (helps manage hypersensitivity to sound, light, and touch)
Social Skills Therapy – social and communication skills – peer based social interaction very beneficial. • Physical Therapy – help with gross motor delays and low muscle tone. • Play Therapy – Need help with learning to play. Good tool for building speech, communication, and social skills. • Behaviour Therapy – Help communicate needs. Help figure out what is behind negative behaviours and to recommend environmental and routine changes needed.
Developmental Therapies – Building on individual’s interests, strengths and developmental level to increase emotional, social and intellectual abilities. • Visually-Based Therapies – Usually involves picture based communication. Video modeling, video games and electronic communication which all address autistic’s visual thinking. • Biomedical Therapies – (Defeat Autism Now – DAN ) Special diets, supplements, and alternative treatments. None are actually approved but have shown some positive outcomes.
GREENSPAN METHOD(FLOORTIME) • Based on social interactions keeping in mind sensory issues. • Dr. Greenspan believes that effective interaction can harness cognitive and emotional growth. • Designed to help achieve six “functional milestones” • Self regulation • Intimacy • Two-way communication • Complex communication • Emotional ideas • Emotional thinking
One-on-one “floor time” for 20-30mins. • Interact and play – spontaneous and fun • Relationship building • 4 goals are: • Encourage attention and intimacy • Two way communication • Encourage expression of feeling and ideas • Logical thought
Applied Behaviour AnalysisABA • Teaches social, motor, verbal behaviours, and reasoning skills. • Positive Reinforcement or Prompting to teach. • Trying to figure out what triggers certain behaviours. • Use to help remove these triggers.
Learning Profile
When looking at the learning profile of an autistic student, it becomes eminently clear that an autistic student is confronting great challenges in learning. All autistic students are capable of learning. As educators, we must remind ourselves that every autistic child learns differently, at a different pace. What may have worked with one student will often not work with the next student.
AUTISM IS A VERY HETEROGENEOUS DISORDER - IF YOU WALK INTO A ROOM OF AUTISTIC INDIVIDUALS YOU ARE OFTEN STRUCK MORE BY THE DIFFERENCES THAN THE SIMILARITIES – Kimberley Ward
Here are some of the challenges: • Most have an uneven profile of skill development due to many of the following factors. • Verbal Communication is limited often only to a few words. Many students with autism will choose to speak only when speaking is initiated by them and useful to them. • Will often have difficulty with the pragmatics of language – knowing what is appropriate to say and understanding the give and take nature of oral communication. (Kutscher)
Will often have difficulty with the semantics of language – the ability to use and understand words, phrases, and sentences, including abstract concepts and idioms. (Kutscher) • Non-verbal communication is unique to the individual, not typical. For example, one student we know makes a variety of signs with his hands and body to express his wants or needs, but these signs are not typical. • In addition, an autistic individual will not necessarily comprehend the facial expressions and body language of others.
Reactive behaviour: Students with autism experience “reactions” (mild flare-ups to explosive behavior) to a variety of circumstances and situations. One might react to sensory issues of sound, light, taste, smell, touch. An illness or lack of sleep may cause a reaction. A reaction is most often due to a lack of anticipation of a stimulus or event. (Bluestone) • Students with autism are resistant to change and may insist on sameness. They need help anticipating change.
Repetitive behaviour is common. Autistic students often have a preoccupation with a particular subject. It is challenging to direct the autistic child to learn about a variety of subjects. • Many students with autism have difficulty with social interaction. The student may find objects more interesting or engaging than people (because they don’t change and, thus, are predictable). An autistic student may not engage in what the teacher or E.A. is teaching because he simply is not connecting to that person. These students have difficulty in joint attention - sharing the same experience as another person.
The Learning Profile of Students with Autism • There is no typical student. All are unique. • All will learn to the best of their abilities. They sincerely give an honest effort. • They need another person to guide them (teacher or E.A.) one-on-one or side-by-side. • They need to trust that the teacher or E.A is on their side – for them, not against them. An autistic student will “bond” with a select few. • They need to trust that the teacher or E.A. is consistent and will prepare them for change or transition.
They need help to anticipate change or new situations and circumstances. • If something works, keep doing it. If it doesn’t, move on to something else. Autistic students, at any given moment, will either have a short attention span or will become intensively focused on finishing a task. • Repetition helps to reinforce learning. • Repetition and consistency gives a feeling of security.
May need more time to learn, or less time. If he doesn’t “get it”, he’ll want to move on. If he “gets it”, he’ll want to move on. A teacher needs to distinguish which is which. An autistic woman, Sue Rubin, writes that “When someone asks me to do something, sometimes I can and other times I can’t. I understand the request but I can’t follow it. I absolutely will eventually be able to do it, but no one waits long enough”. (Savarese) • Access to a computer is helpful. Most computer programs are predictable. Also, typing is easier than printing.
Autistic students are often kinesthetic learners – learn through movement – and physical activity is helpful in engaging, motivating and relaxing them. • Many autistic students respond positively to music. • Many autistic students will communicate in a variety of ways. Non-autistic people need to understand those various ways of communication. For example, unusual word patterns, sounds, body language, written words, using the specific language of “talkers”. (Dynavox, Minspeak, etc.)
Speaking via a “talker” or through written words is self-esteem building and liberating. • All behaviour is communication. • There is “autistic introspection”. Many autistic people dispute the “theory of mind” philosophy. (Savarese)
More and more people with autism are opening up publically about their experiences: Judith Bluestone, Temple Grandin, Tito Mukhopadhyay, Sue Rubin, and the list goes on. As educators, we need to learn (and teach) through their experiences of autism, not ours. James Charlton, an historian of the global disability rights movement insists, “Nothing about us without us.” (Savarese)
Classroom/School • Problem – bright lights, noises, people, objects • Some or all can cause confusion, upset or over excitement. • Removal or desensitization over time • Provide a relaxation area or relaxation object such as stress ball, stuffed toy, ball of string etc. for calming
Desensitization • Problem – anxieties, fears, obsessions, rituals • Gradually have rehearsals and exposure to items or activities that cause anxieties, obsessions, etc then give reinforcement. • Show clues, provide cues, to prepare for upcoming events.
Routines and Schedules • Problem - insecurity and lack of order • Provide visual guides: calendars, schedules, picture boards etc. • All present an abstract concept of time in a concrete, manageable form. • The results are order and security
Augmentative Communication • Problem – minimal or no communication • Sign language, communication boards, electronic devices • Enable communication so need to be used in all settings in order to communicate their wants and needs
Visual Cues • Problem – need for guidance and/or reassurance • Use of learning guides in the form of cue cards, list of steps and procedures. Maybe small ie. on recipe cards or large displays on bulletin boards.
Stimulus Cues • Problem – confusion often occurs due to difficulty processing verbal instruction or anticipating routines • Rehearse cue and clues to help alleviate confusion • eg. Rehearse routine and discuss event • i.e. getting placemat = lunchtime • getting umbrella = raining • getting keys = going out