Download
1 / 44
460 likes | 679 Views
Integumentary System. Disclaimer. There may be images that are uncomfortable for you. My apologies, however, I feel real human photos (when available) are more educational. Objectives. Define system Identify structures of system Identify anatomy of structures

E N D
Disclaimer • There may be images that are uncomfortable for you. • My apologies, however, I feel real human photos (when available) are more educational.
Objectives • Define system • Identify structures of system • Identify anatomy of structures • Understand functions of structures • Know pathology of structures
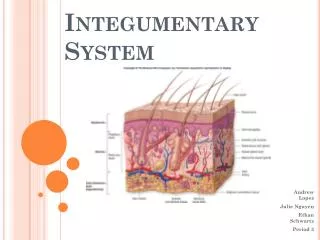
Integumentary system • Skin • Hair • Nails • Exocrine glands
Skin – Epidermis = superficial section • 40-50 row of stacked squamous epithelial cells • Contains zero blood vessels • Nutrients from dermis • 90% made up of Keratinocytes • Keratin makes this rough and water resistant • 8% made up of Melanocytes • Produces pigment (melanin) for protection • >1% made up of Langerhans cells • Detect and fight pathogens • <1% made up of Merkel cells • Sense touch
Papillary layer of dermis (dermal papillae) supplies nutrients and oxygen to epidermis – touch, pain and temperature Dermis = middle section
Reticular layer of dermis – collagen and elastic = strength and elasticity
Hypodermis – deepest section • AKA subcutaneous tissue or superficial fascia • Collagen, elastic, fatty adipose tissue • Energy reservoir and thermal insulation • Site for hypodermic injections = highly vascular
Hair = accessory skin organ Keratinocytes = hair Melanocytes = hair color
Nails Nain = hardened keratinocytes Distal edge = free edge Bed = epidermis and dermis below Root = nail matrix Cuticle/eponychium = seals nail to protect from infection
= organs that produce secretions that must exit a gland through a duct
Thermoregulation Sweat glands = sudoiferous glands Apocrine – axilla and pubic regions active beginning with puberty, oily liquid = odor Eccrine = Merocrine = water and sodium chloride delivered to the skin
Sebaceous Gland Oily secretion = sebum Sebum = lubricates cuticles, of hair water proof and provide elasticity Everywhere EXCEPT: palms of hands and soles of feet
Ceruminous Glands Found only in dermis of ear canals Waxy secretion = cerumen Cerumen = protect and lubricate ear canals Made consistently and pushed out of external ear or removed manually
Pathologies • Bacterial Infections • Environmental skin responses • Fungal Infections • Inflammatory skin responses • Mechanical trauma • Parasitic Infections • Viral Infections • Misc.
Bacterial Infections - contagious • Community-Acquired Methicillin-Resistant Staphylococcus aureus (CA-MRSA) • Pimple-like lesions, pustules, or boils • May infect existing cuts and abrasions • Risk factors: • Close skin to skin contact (wrestling) • Contaminated items such as towels (ATR/locker room) • Crowding (elevators) • Cleanliness (freshman ) • Compromised skin integrity • Prevention: • Wash, don’t share, cover, refer, use proper first aid procedures • Treatment: • IV, antibiotics, hospitalization
Bacterial Infections - contagious • Impetigo • Honey-colored, crusted, well-defined vesicles • Most commonly on fact and other exposed areas • Athletes with moist, crusted lesions = hold from participation • Athletes with dried, crusted lesions, have completed 5 days of antibiotics, and no new lesions within 48 hours = may participate • Do not cover ACTIVE lesions to participate • Cover inactive lesions with nonpermeable dressing • Must rule out MRSA
Bacterial Infections – may worsen with activity • Cellulitis • Involves the skin and subcutaneous tissue • Occur at site of previous wound • Takes serval days to develop • Raised, well-defined, expanding, red plaque • Redness, swelling and warmth at site • May include fever and malaise • Erysipelas • Involves epidermis and upper portion of dermis • Raised, well-defined, expanding, red plaque • May include fever and malaise • Treatment of antibiotics, may need to drain • RTP = same as impetigo
Bacterial Infection Cellulitis Erysipeals
Bacterial Infections – may worsen with activity • Furuncles AKA boils – contagious only if infected • Tender, red nodules that contain a core of necrotic tissue and pus • Open wounds are at risk for this • Single furuncle treat with moist, hop compress • Carbuncles • Clusters of furuncles • Treatment/RTP – complete at least 5 days of treatment, no draining or moist lesions and no new lesions within 48 hours
Bacterial Infections Furuncle Carbuncle
Bacterial Infections – no risk • Folliculitis • Caused by friction of clothing or equipment • Extensive cases involve deep portion of hair follicle • Redness and tenderness • “hot tub” folliculitis – 2 to 3 days post exposure, lasts for 7- 10 days on skin of swimsuit area • May have fever, nausea, vomiting, headache, pharyngitis and otitis externa • Treatment – oral antibiotics • RTP – no limitations
Fungal Infections • Topical named for location or by description • *Tinea pedis – feet • Tinea cruris – “jock itch” – groin (tight clothes, obesity) • Tinea unguium – finger and toenails (diabetes, age) • *Tinea corporis – head/arms/neck = ringworm = tinea gladiatorum • Tinea versicolor – back/trunk/abdomen/arms – change in pigment and high rate of recurrence • Prevention: shower shoes, keep clean, area dry, skin screening, prophylactic anti-fungal dosing • Treatment: most can use topical antifungal powder or cream – apply 2cm beyond the lesion, some may need oral anti-fungal medication • * contagious
Inflammatory Skin Responses • Acne Vulgaris • Hair follicle or sebaceous gland blocked, accumulates serum = immune system responds = pustules, then rupture = inflammation extends down in to the dermis • Mild = 3-10 lesions • Moderate = 10 – 30 lesions • Severe = > 30 lesions • Non-inflammatory = black heads and pimples • Inflammatory = cysts and nodules
Inflammatory Skin Responses • Contact Dermatitis • Allergic contact (poison ivy) • Changes in bath soap or laundry detergent • Other common allergens • Rubber products • Topical creams • Athletic tape or adhesive spray • Epoxy (face gear) • Fiberglass • Treatment – Claritin (non-drowsy) or Benadryl (sedative)
Inflammatory Skin Responses Eczema = chronic dermatitis Plaque Psoriasis - silver like scales
Environmental Skin Responses Urticaria (cold, cholinergic, solar) Raynaud’s syndrome
Environmental Skin Responses Normal frostnip superficial frostbit deep frostbite
Environmental Skin Responses 1st degree sunburn 2nd degree sunburn
Mechanical Trauma • Blisters – moisture and friction • Calluses – repetitive friction • Acne Mechanica – pressure, friction, heat and occlusion (often under equipment) • Talon Noir = black heel (bluish-black dots), lateral shearing forces cause intra-epidermal bleeding. If persistent black dots, have checked for melanoma
Viral Infections • Spread requires direct skin contact with infected lesions • Prevention – cover all abrasion and open wounds, regular skin screening • Herpes Simplex Virus (HSV) • Type 1 Type 2 - genital
Viral Infections • Herpes Labialis = cold sore or fever blister • Causes = sun, physical or emotional stress • Tingling or burning prior to appearance of lesion • Treatment = OTC’s • RTP = asymptomatic, no new lesions for 3 consecutive days, all lesions are crusted and athlete has taken appropriate dos of a systemic antiviral medication for at least 5 days
Viral Infections • Herpes Gladiatorum • Commonly affects wrestlers = “gladiator” • Clustered vesicular lesions on an erythematous base • Itching or burning prior to appearance • Possible systemic symptoms • Fever, chills, headache, sore throat, malaise • Treatment and RTP = same as herpes labialis • Ocular HSV = blindness • Refer immediately if lesions appear near eyes
Viral Infections • MolluscumContagiosum • Spread by direct skin contact and sexual contact so can be categorized as a STD • Rash, white, pinkish, or skin colored, dome-shaped papules with a center dimple • NCAA requires these to be removed from wrestlers prior to participation
Viral Infections • Warts • Caused by HPV • Contagious – skin to skin or by contaminated surface • Treatment – destroy by freezing, burning, electrocautery or topical acid • RTP – no loss of time but must be covered
Viral Infections Varicella - Chicken pox Herpes Zoster - Shingles
Parasitic Skin Responses • Lice • Head, body, pubic (“crabs”) • Scabies • Insect bites • Necrotic arachnidism = results from the brown recluse spider (AKA fiddle-back spider) venom • Photo deleted in case anyone suffers from arachnophobia
Misc. • Alopecia – baldness • Hirsutism – excessive hair growth • Onychia– infection of the nail bed or nail matrix • Viral or fungal • Paronychia – infection affects the proximal or lateral nail fold • Viral or fungal