Download
1 / 1
10 likes | 165 Views
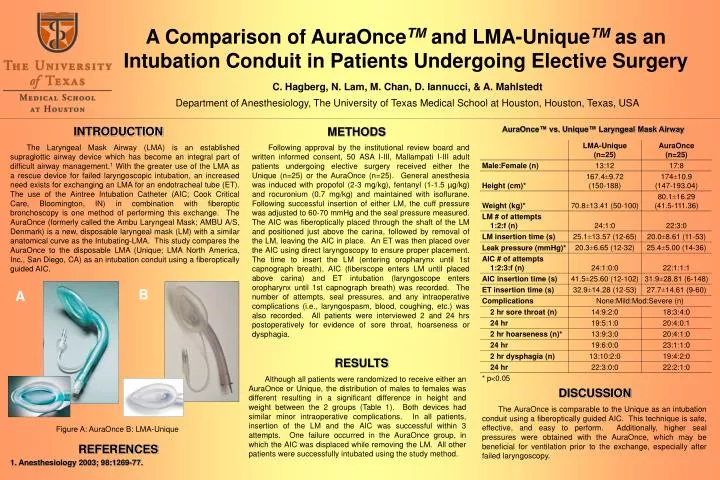
A Comparison of AuraOnce TM and LMA-Unique TM as an Intubation Conduit in Patients Undergoing Elective Surgery. INTRODUCTION. AuraOnce™ vs. Unique™ Laryngeal Mask Airway. METHODS.

E N D
A Comparison of AuraOnceTM and LMA-UniqueTM as an Intubation Conduit in Patients Undergoing Elective Surgery INTRODUCTION AuraOnce™ vs. Unique™ Laryngeal Mask Airway METHODS The Laryngeal Mask Airway (LMA) is an established supraglottic airway device which has become an integral part of difficult airway management.1 With the greater use of the LMA as a rescue device for failed laryngoscopic intubation, an increased need exists for exchanging an LMA for an endotracheal tube (ET). The use of the Aintree Intubation Catheter (AIC; Cook Critical Care, Bloomington, IN) in combination with fiberoptic bronchoscopy is one method of performing this exchange. The AuraOnce (formerly called the Ambu Laryngeal Mask; AMBU A/S, Denmark) is a new, disposable laryngeal mask (LM) with a similar anatomical curve as the Intubating-LMA. This study compares the AuraOnce to the disposable LMA (Unique; LMA North America, Inc., San Diego, CA) as an intubation conduit using a fiberoptically guided AIC. Following approval by the institutional review board and written informed consent, 50 ASA I-III, Mallampati I-III adult patients undergoing elective surgery received either the Unique (n=25) or the AuraOnce (n=25). General anesthesia was induced with propofol (2-3 mg/kg), fentanyl (1-1.5 µg/kg) and rocuronium (0.7 mg/kg) and maintained with isoflurane. Following successful insertion of either LM, the cuff pressure was adjusted to 60-70 mmHg and the seal pressure measured. The AIC was fiberoptically placed through the shaft of the LM and positioned just above the carina, followed by removal of the LM, leaving the AIC in place. An ET was then placed over the AIC using direct laryngoscopy to ensure proper placement. The time to insert the LM (entering oropharynx until 1st capnograph breath), AIC (fiberscope enters LM until placed above carina) and ET intubation (laryngoscope enters oropharynx until 1st capnograph breath) was recorded. The number of attempts, seal pressures, and any intraoperative complications (i.e., laryngospasm, blood, coughing, etc.) was also recorded. All patients were interviewed 2 and 24 hrs postoperatively for evidence of sore throat, hoarseness or dysphagia. C. Hagberg, N. Lam, M. Chan, D. Iannucci, & A. Mahlstedt Department of Anesthesiology, The University of Texas Medical School at Houston, Houston, Texas, USA B A RESULTS Although all patients were randomized to receive either an AuraOnce or Unique, the distribution of males to females was different resulting in a significant difference in height and weight between the 2 groups (Table 1). Both devices had similar minor intraoperative complications. In all patients, insertion of the LM and the AIC was successful within 3 attempts. One failure occurred in the AuraOnce group, in which the AIC was displaced while removing the LM. All other patients were successfully intubated using the study method. DISCUSSION The AuraOnce is comparable to the Unique as an intubation conduit using a fiberoptically guided AIC. This technique is safe, effective, and easy to perform. Additionally, higher seal pressures were obtained with the AuraOnce, which may be beneficial for ventilation prior to the exchange, especially after failed laryngoscopy. Figure A: AuraOnce B: LMA-Unique REFERENCES 1. Anesthesiology 2003; 98:1269-77.