Download
1 / 51
580 likes | 1.67k Views
Visualization of the cervix with acetic acid and Lugol’s iodine to improve sensitivity of detecting cervical dysplasia. Instruction material adapted from: International Agency for Research on Cancer ( IARC ) World Health organization (WHO) Program for Appropriate Technology in Health (PATH)

E N D
Visualization of the cervix withacetic acid and Lugol’s iodineto improve sensitivity of detecting cervical dysplasia Instruction material adapted from: International Agency for Research on Cancer (IARC) World Health organization (WHO) Program for Appropriate Technology in Health (PATH) ASCCP
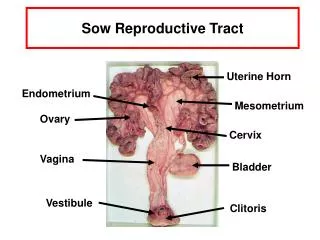
Outline • Anatomy of the cervix • Procedure: visualization of the cervix with acetic acid and Lugol’s iodine • Identifying lesions • VIA-negative • VIA-positive • Invasive carcinoma • Epic documentation for data collection.
Cervical epithelium • Squamous epithelium • Vagina and outer ectocervix • Columnar epithelium • Upper and middle endocervical canal • Squamous metaplasia = transformation zone • Central ectocervix and lower endocervical canal *Almost all cervical neoplasia occurs in the transformation zone
Transformation zone The area of the cervix between the original and the new sqamocolumnar junction Where the columnar epithelium has been replaced or is being replaced by the metaplasticsquamous epithelium.
Original Squamocolumnar Junction • Placement determined between 18-20 weeks gestation • Childhood and perimenarche it is located at or very close to the cervical os. • After puberty the endocervical canal elongates. This leads to the eversion of the columnar epithelium onto the ectocervix, resulting in ectropion or ectopy. • (Can be found in vagina or vaginal fornices in DES exposed women) • Less apparent over time with maturation of epithelium
Squamous metaplasia • Progressive replacement of columnar epithelium by squamous epithelium • Stimulated by • Acidic environment with puberty • Obliteration of original columnar cells • Subsequent maturation into well-differentiated, glycogenated squamous epithelium
New “SCJ” As metaplastic changes occur, the location of the SCJ moves on the ectocervix towards the cervical os During menopause the cervix shrinks due to the lack of estrogen, resulting in the progression of the SCJ into the endocervical canal Adequate colposcopy requires visualization of the entiresquamocolumnar junction
Transformation zone The area of the cervix between the original and the new sqamocolumnar junction where the columnar epithelium has been replaced or is being replaced by the metaplasticsquamous epithelium. With the naked eye, one can identify the inner border of the transformation zone by tracing the squamocolumnar junction and the outer border by locating the distal most nabothian cysts (if present) or crypt openings. Majority of dysplasia is in the transformation zone or the leading edge of the squamousmetaplasia, abutting the SCJ.
Visualization inspection tests • Visual inspection with acetic acid (VIA)done with the naked eye also called cervicoscopy or direct visual inspection [DVI], or with low magnification called gynoscopy, aided VI, or VIAM. • Visual inspection with Lugol’s iodine (VILI),also known as Schiller’s test
Visualization of the cervix with acetic acid (VIA) When to perform? • Anytime during the menstrual cycle including during menses (providing flow is not too heavy) • During pregnancy, at a postpartum examination • For STI screening • Intended for ages 20 to 50
VIA test performance: Source: Adapted from Gaffikin, 2003 Pap test performance: These results are from a meta-analyses of cross-sectional studies (US department of health and human services Agency for Health Care Research and Quality 1999). Several ACCP studies have also found Pap test sensitivity in the range of 50% at best.
Preparing for VIA(at Swedish Family Medicine) Provide the explanation of the procedure in writing at the time of rooming. “opt out” policy Additional equipment needed for set up: • Reporting form, “dot phrase” (Epic based) • Cotton swabs which are soaking in cups of • 5% acetic acid (white table vinegar) • Lugol’s iodine solution
Patient information (draft) Patient Handout for VIA Project Cervical cancer affects over 10,000 women in the U.S. each year. Our clinic is doing a project that may improve our ability to detect abnormalities of the cervix before they turn into cancer. In addition to doing a pap smear today, we would like to put vinegar and an iodine solution on your cervix to look for abnormalities that a pap smear might miss. You will probably not even notice that the doctor is doing this extra step. There are no side effects, but it may add about 5 minutes to your visit. You may also have some discharge that is iodine-color (brown). If we see anything abnormal with this exam, or if your Pap smear is abnormal, we will recommend that you schedule a colposcopy. A colposcopy is a procedure in which we take a closer look at your cervix. If we still see any abnormal areas during the colposcopy, we may recommend taking a sample (biopsy) of your cervix. Ask your doctor if you have questions about this procedure. Please let your doctor know if you do not want us to do take a closer look at your cervix using these solutions, or if you have an allergy to iodine. Thank you for helping us to improve the quality of care we provide to our patients!-Drs - Alyson Feigenbaum (at large) and Xandra Rarden.
Procedure *prior to application of acetic acid • Inspect the external genitalia: papules, vesicles, ulcerations, condylomata, discharge, redness, swelling, excoriation. • Inspect the cervix: cervicitis, nabothian cysts, ulcers, condylomata, polyps, leukoplakia (thickened, white patches), vesicles, papules, or ulcers on the cervix, easy bleeding? • Perform Pap and HPV test as indicated • Perform wet mount and STI screening as indicated • Use a dry cotton swab to wipe away any discharge, blood, or mucus from the cervix.
Procedure involving VIA and VILI • Soak a clean swab in 5% acetic acid and apply to the cervix liberally. • Wait 1 minute. Tell the woman that she might feel a slight burning sensation especially if the tissue looks inflamed or friable. • Focus your view on the transformation zone. • Note any acetowhite lesions: location, extension, intensity of whiteness, borders. • Soak a clean swab in Lugol’s iodine solution and apply to cervix liberally • Note the uptake in the areas of concern noted after acetic acid.
Pathophysiological basis of VIA Application of 5% acetic acid causes: • A reversible coagulation of the cellular proteins which obscures the color of the underlying stroma. Thus the increased nuclear activity and DNA content exhibit the most dramatic white color change • swelling of the epithelial tissue • dehydration of the cells and clearing the mucous secretions on the cervix.
Glycogen-containing tissue stains mahogany brown or black Glycogen rich: Squamous epithelium Squamous metaplasia Glycogen poor tissues do not take up iodine and appear mustard-yellow or saffron-colored areas. Glycogen poor: Columnar epithelium CIN and invasive cancer Laukoplakia (hyperkeratosis) condylomata Pathophysiological basis of VILI Lugol’s iodine is glycophillic
Reporting of lesionsVIA negative No significant acetowhite lesions. This is the most challenging category in VIA because there are many variations of acetowhite areas that can appear. Closely consider: Nabothian cysts and polyps may also turn acetowhite There may be a faint line, appearing to be acetowhitening at the junction of columnar and squamous epithelium. There may be acetowhitelesions far away from the squamocolumnar junction or streaklikeacetowhitening. There may also be dotlike areas on the columnar epithelium, which are due to areas of metaplasia Diffuse acetowhiteningwith columnar epithelium staining
VIA-negative VIA negative. The mild acetowhite staining in a linear pattern at the lower edge of the squamocolumnar junction and around the two glandular crypt openings is the typical appearance of immature metaplasia. Used with permission from Program for Appropriate Technology in Health (PATH). Seattle, WA: PATH.
VIA-Negative There are no acetowhite areas on the polyp and the cervix after the application of acetic acid. No acetowhite area seen. Note the advancing edges of squamous metaplasia in the anterior and posterior lips (arrows).
VIA-negative VIA negative. The button-like, acetowhite area with ill-defined margins is due to a Nabothian cyst. Other ill-defined acetowhite areas are due to squamous metaplasia. (Program for Appropriate Technology in Health (PATH). Seattle, WA: PATH.)
VIA-negative The nabothian cysts appear as pimple- or button-like areas after the application of acetic acid. There is dot-like acetowhitening in the columnar epithelium in the anterior lip. The squamocolumnar junction is fully visible.
VIA-negative There is an ill-defined pinkish-white hue with indefinite margins blending with the rest of the epithelium. The squamocolumnar junction is fully visible.
VIA-negative • There is dense, thick, mucus on the cervix before the application of acetic acid. After the application of acetic acid, the mucus is cleared and the squamocolumnar junction becomes prominent.
Inflammation of the cervix - cervicitis Common agents: Trichomonas, Candida albicans, anaerobes (Gardnerella vaginalis, G. mobilluncus and peptostreptococcus) Neisseria gonorrhea, Chlamydia trachomatis, Escherichia coli, streptococci, staphylococci, herpes simplex Columnar epithelium is more prone to infection than squamous epithelium. Pay attention to symptoms: excessive discharge, itching of the vulva and vagina, pain and a burning sensation during sexual intercourse and lower abdominal pain
Visual inspection-cervicitis Candidial: vulvar edema and erythema, excoriation, and thick, curdy-white, non-odorous discharge. Non-candidial: vulval erythema and edema, reddish, tender cervix with malodorous, greenish yellow or greyish-white mucopurulent discharge, with or without ulceration. Gonococcal: painful urethral discharge is also observed. Herpes infection: vesicles and ulcers in the external genitalia, vagina and the cervix, as well as cervical tenderness.
VIA-negative The cervix is unhealthy, inflamed with ulceration, necrosis, bleeding and inflammatory exudate.There is ill-defined, diffuse, pinkish-white acetowhitening with indefinite margins blending with the rest of epithelium (arrows).
VIA-Positive Pay attention to: Sharp, distinct, well-defined, dense (opaque/dull or oyster white) acetowhite areas, with or without raised margins, close to the squamocolumnar junction.
Other conditions • Condylomatafound on the cervix, and occasionally in the vagina and on the vulva, associated with HPV types 6 and 11. Condylomata are usually obvious to the naked eye (before the application of acetic acid).
Other conditions • Leukoplakia(hyperkeratosis) is a well demarcated white area on the cervix (before the application of acetic acid), due to keratosis, visible to the naked eye. Usually leukoplakia is idiopathic, but it may also be caused by chronic foreign body irritation, HPV infection, or squamous neoplasia.
VIA-Positive moderately opaque, sharply bordered, wide band of acetowhite staining around the cervical os, touching the squamocolumnar junction. There is mild acetowhite staining of the immature metaplastic epithelium extending onto the endocervical polyp. (Program for Appropriate Technology in Health (PATH). Seattle, WA: PATH.)
VIA-positive There is a well-defined, opaque acetowhite area, with irregular digitating margins, in the anterior and posterior lips abutting the squamocolumnar junction and extending into the cervical canal. There is a well-defined, opaque acetowhite area, with bleeding on touch, in the anterior lip, abutting the squamocolumnar junction, which is fully visible.
VIA-positive There is a well-defined, opaque acetowhite area, with regular margins, in the anterior lip, abutting the squamocolumnar junction, which is fully visible. Note the satellite lesions in the lower lip. There is a well-defined, opaque acetowhite area, with regular margins, in the anterior lip, abutting the squamocolumnar junction, which is fully visible. Note the somewhat ill-defined white area in the lower lip. The lesion is extending into the cervical canal.
VIA-positive There is a well-defined, dull, dense, opaque acetowhite area in the posterior lip extending into the endocervical canal. There is an acetowhite area in the columnar epithelium in the anterior and posterior lips.
VIA-positive There is a dense acetowhite area all over the cervix involving all the four quadrants and extending into the cervical canal.
Invasive cancer Early lesions may present as a rough, reddish, granular area that bleeds on touch
Invasive cancer There is a dull, opaque, dense acetowhite area, with raised and rolled-out margins, irregular surface and bleeding on touch in the posterior lip. The lesion is extending into the cervical canal. The bleeding obliterates acetowhitening. There is a proliferative growth with dense acetowhitening and bleeding
Invasive cancer There is a dense acetowhite area with irregular surface contour. There is an ulceroproliferative growth with acetowhitening and bleeding
Invasive cancer More advanced cancers may present as a proliferating, bulging, mushroom- or cauliflower-like growth with bleeding and foul-smelling discharge
Distribution of findings A sufficiently skilled examiner will categorize 8-15% of women examined as VIA-positive 20-30% of the VIA-positive lesions identified on VIA by the test provider harbor CIN of any grade
Epic dot phrase: The first block of information would be entered by the “data enter” only. • Location of clinic (standard clinic, medical home model) • Data collection: • Date of service • Name • Age • Type of visit **************************************** • Pap results • Colposcopy results
Epic dot phrase Added to the chart note: • Did the patient agree to have VIA after reading the information provided? Y / N / *** • Did the patient have any concerns about this test? Y / N / *** • How long did you spend counseling the patient about this supplemental test? 1/3/5/10/*** minutes • Findings: VIA negative / VIA positive / neoplasm • Lugol’s iodine used Y / N / *** • Evidence of cervicitis on exam Y / N, tested Y / N, treated Y / N • Screening for SDIs Y / N • Pap done? Y/N • HPV done? Y/N
Epic dot phrase • Were VIA results discussed with the patient? Y / N • Was colposcopy recommended at the time of the screening test? Y / N • If yes, did the patient elect to schedule colposcopy or wait for pap results? *** • If yes, what concerns did the patient have about undergoing colposcopy? *** • Was this test uncomfortable for the patient in any way? • No / yes it was physically uncomfortable / patient felt psychologically uncomfortable about visualizing the cervix / the patient felt that it took time away from the rest of the visit / *** • Was the provider uncomfortable in any way? • No / the provider felt uncomfortable counseling the patient / performing the visualization / making recommendations / ***