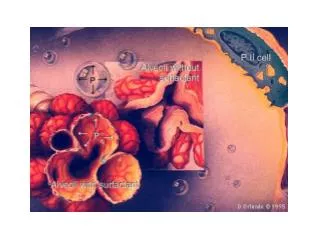
Download
1 / 79
910 likes | 1.76k Views
Respiratory Diseases in Children. Christine T. Quien-Sua, MD DPPS DPAPP Pediatric Pulmonology January 18, 2010. Respiratory System: Upper respiratory tract Lower respiratory tract. Choanal atresia Foreign body Common cold Sinusitis Pharyngitis

E N D
Respiratory Diseases in Children Christine T. Quien-Sua, MD DPPS DPAPP Pediatric Pulmonology January 18, 2010
Respiratory System: • Upper respiratory tract • Lower respiratory tract
Choanal atresia Foreign body Common cold Sinusitis Pharyngitis Retropharyngeal/ lateral pharyngeal abscess Laryngomalacia Croup Acute Epiglotittis Obstructive Sleep Apnea Upper Respiratory Tract Disorders
Choanal Atresia • Most common congenital anomaly of the nose • Bony (90%) or membranous (10%) septum • CHARGE syndrome - Coloboma, Heart , Atresia, Retarted growth, Genital and Ear • Clinically unilateral - asymptomatic bilateral - difficulty in breathing with cyanosis relieved when crying
Choanal Atresia • Diagnosis: inability to pass a catheter through each nostril 3-4 cm into the nasopharynx rhinoscopy or HRCT scan • Treatment: • Supportive: oral airway, intubation or tracheostomy; NGT • Definitive: Surgery
Foreign Body (Nose) • Symptoms: • Local obstruction, sneezing, mild discomfort, pain • Disk batteries – most dangerous because it leach in matters of hours • Diagnosis: • Unilateral nasal discharge and/or obstruction • Nasal speculum/ otoscope • Complications: • Tetanus • Toxic shock syndrome
The Common Cold • Most common upper respiratory tract infection (AURI), rhinitis, nasopharyngitis • Viral illness • Rhinovirus - the most common pathogen • Coronavirus, RSV • 6-7 colds / year • 10-15% of children have at least 12 infections per year
The Common Cold • Sore or “scratchy” throat • Nasal obstruction • Rhinorrhea • Cough • duration - 1 week • 10% - last for 2 weeks
Common cold • P.E. limited to the upper respiratory tract • A change in color or consistency of the secretions is common during the course of illness and is NOTindicative of sinusitis or bacterial superinfection
Table 364-2 Conditions that May Mimic the Common Cold p. 1390 Nelson Textbook of Pediatrics 17th ed p
The Common Cold: Treatment • Fever - acetaminophen • Nasal obstruction -adrenergic agents as decongestants • Rhinorrhea - first generation anti-histamine due to the anticholinergic effect • Sore throat - mild analgesics • Cough - due to postnasal drip; due to virus-induced reactive airway disease-antihistamine/bronchodilator
The Common Cold: Treatment Ineffective Treatments: • Vitamin C • Guaifenesin • Inhalation of warm, humidified air • Zinc • Echinacea -herbal treatment
Common cold: Complications • Otitis media - most common • Sinusitis • Asthma exacerbation • Inappropriate us of antibiotics – antibiotic resistance
Sinusitis • Etiology: viral or bacterial • Clinical signs suggestive of acute bacterial sinusitis • Persistent signs/symptoms of URTI of > 14 days without improvement • Severe respiratory symptoms (e.g. temp >39 C) • Purulent nasal discharge for 3-4 consecutive days • Common bacterial pathogens of acute sinusitis Streptococcus pneumonia H. influenza Moraxella catarrhalis
Sinusitis • Persistent symptoms of URI – nasal congestion/discharge, fever & cough • Less common symptoms: halithosis, decreased sense of smell, periorbital edema • P.E. mild erythema/swelling of nasal mucosa with nasal discharge • Sinus tenderness in adolescents
Diagnosis: Sinusitis • Transillumination of sinus cavities • Sinus plain films and CT scan • Opacification, mucosal thickening, presence of air-fluid level • Sinus aspirate culture • not practical for routine use
Sinusitis - Treatment • Amoxicillin (45mkday) • Amoxicillin-clavulanate (80-90mkday) • Cephalosphorins • Clarithromycin, Azithromycin • Duration: continue for 7 days after resolution of symptoms
Sinusitis - Complications • Eye complications: • peri-orbital/ orbital cellulitis • Intracranial complications: • Meningitis • cavernous sinus thrombosis • abscess
Acute pharyngitis • Etiology: Group A beta-hemolytic Streptococcus (GABHS) , virus • Uncommon before 2-3 years old • Peak incidence: 4-7 years old • Sore throat as the primary symptom
Viral pharyngitis • Presence of 2 or more of these signs and symptoms suggest viral infection: • Conjuctivitis - stomatitis • Rhinitis - discrete ulcerative lesions • Cough - viral exanthem • Hoarseness diarrhea • Coryza
Streptococcal pharyngitis • M protein- major virulence factor that resists phagocytosis • Physical examination: • red pharynx • enlarged tonsils with yellow blood-tinged exudate • petechiae on the soft palate and posterior pharynx • enlarged/tender anterior cervical lymph nodes • Diagnosis: Throat culture - gold standard
Treatment • Penicillin V -250mg/dose bid or tid x 10 days • Amoxicillin - 750mg OD x 10d 50mkday bid x 6 days • Benzathine Pen IM - 600,000 U for < 27kgs - 1.2M units • Erythromycin 40mkday tid or qid x 10days
Strep. pharyngitis • Prevention of acute rheumatic fever is successful if treatment started within 9 days of illness • Clindamycin (20mkday) - recommended for carriers
Retropharyngeal and lateral pharyngeal abscess • ETIOLOGY: • Complication of bacterial pharyngitis • Extension of infection from vertebral osteomyelitis • Dental infection • Trauma • Group A hemolytic strep., anaerobes, Staph. aureus
Retropharyngeal and lateral pharyngeal abscess • Clinical manifestations: • With hx of acute nasopharyngitis • Abrupt onset of fever, difficulty of swallowing, refusal to feed, severe distress with throat pain, hyperextension of head, drooling • P.E. • Bulge in posterior pharyngeal wall
Retropharyngeal and lateral pharyngeal abscess • Lateral x-ray of the neck • Retropharyngeal soft tissue is thick • Retropharyngeal air • Loss of N cervical lordosis • Treatment • IV antibiotics with or without surgical drainage • 3rd gen cephalosporins+ Sulbactam-ampi or Clindamycin
Laryngomalacia • Most common congenital laryngeal anomaly • Most frequent cause of stridor in infants and children • Stridor appear at 2 weeks of life • Increase in severity up to 6 months • Diagnosis: flexible bronchoscopy • Treatment: observation - spontaneously resolve
Acute Inflammatory Upper Airway Obstruction Viral agents accounts for most acute infectious upper airway obstructions except in: Diphtheria Bacterial tracheitis Acute epiglottitis
Laryngotracheobronchitis (Croup) • Heterogeneous group of mainly acute and infectious processes • brassy or bark-like cough • hoarseness, inspiratory stridor, respiratory distress • Parainfluenza viruses (type 1,2,3) - 75% of cases • age group: 3 mos - 5 y/o • peak 2y/o • Diagnosis is clinical
Soft tissue neck radiograph Laryngotracheobronchitis Epiglotittis “steeple sign” “thumb sign” Postero-anterior view lateral view
Croup -Treatment • Airway • Cool mist • Nebulized racemic epinephrine 0.25 to 0.75mL of 2.25% of epi in 3mL NSS q 20mins duration < 2 hrs • Corticosteroids Dexamethasone IM - 0.6mg/kg single dose or 0.15mg/kg Budesonide nebulized - 2mg • Helium-oxygen mixture
Acute Epiglottitis • Etiology: H. influenza type B • Clinically: high grade fever, fever, rapidly progressing dyspnea • barking cough is rare • PE: “cherry red”epiglottis • lateral radiograph of the upper airway
Treatment • Establish the airway! • Don’t forget oxygen • Ceftriaxone, cefotaxime, sulbactam-ampi for 7-10 days • Rifampicin prophylaxis (20mg/kg OD x 4 days)
Bacterial Tracheitis • Complication of a viral disease • Life-threatening • < 3 years old • High grade fever, brassy cough, respiratory distress, “toxic” BUT does NOT drool and no dysphagia and can lie flat in bed • copious purulent secretions with pseudomembrane • mucosal swelling at the level of cricoid cartilage • Etiology : Staphylococcus aureus • Treatment: Airway, antibiotics and O2 support
Obstructive Sleep Apnea DEFINITION: • Disorder of breathing during sleep with prolonged partial upper airway obstruction and/or intermittent complete obstruction that disrupts normal ventilation during sleep
OSA • Prevalence rate: 0.7% -3% • Peak: preschool (2-5y/o) male = female • Adenotonsillar hypertrophy – the most common anatomic predisposing factor • REM sleep – the most common functional predisposing factor
OSA • No direct correlation between tonsil size and severity of OSA. • Habitual snoring – most common symptom • Triad of symptoms: • Snoring • Nocturnal breathing difficulties • Witnessed respiratory pauses
OSA • Overnight recording of multiple physiologic sensors during sleep (POLYSOMNOGRAPHY) – gold standard for diagnosis • Treatment: Adenotonsillectomy • Complications if untreated: • Failure to thrive • Pulmonary hypertension • Cor pulmonale
Disorders of the Lower Respiratory Tract • Foreign body aspiration • Bronchitis • Bronchiolitis • Pneumonia • Bronchial Asthma • Pneumothorax • Acute Respiratory Distress Syndrome
Foreign Body Aspiration • Older infants and toddlers • With or without history of choking • May present with wheezing, stridor, chronic cough • Most common : peanuts • Chest x-ray: air trapping, atelectasis • Rigid bronchoscopy – diagnostic and therapeutic
Acute Bronchitis • Protracted cough lasting for 1-3 weeks • Damaged or hypersensitized tracheobronchial epithelium • Preceded by a viral URTI • afebrile, cough ( dry or purulent) , chest pain • PE: coarse and fine crackles , wheezing • Chest xray: Normal or increase bronchial markings • IMPORTANT to exclude pneumonia • Self - limited and require NO treatment
Acute Bronchiolitis • Common disease of the lower respiratory tract in infants • Age group: 3 months - 2 y/o • Etiology: Respiratory syncytial virus (RSV) • Clinical: fever, rhinorrhea --- gradual respiratory distress, dyspnea and irritability • Absence of other systemic complaints as diarrhea or vomiting
Acute Bronchiolitis • PE: tachypnea, nasal flaring, retractions predominantly wheezing • Chest radiograph: hyperinflation with patchy atelectasis
Bronchiolitis-Treatment • The first 48-72hrs after onset of cough and dyspnea is the most critical • Humidified O2 • Position - head and chest elevated and neck extended • NPO and IV fluids • Bronchodilators and nebulized epinephrine • Ribavirin - thru aerosol tx used for infants with CHD and chronic lung disease • Corticosteroid and antibiotics - NO benefit