Download
1 / 1
10 likes | 145 Views
Importance of a prostate cancer registry for describing changing patterns of care. No. 094.

E N D
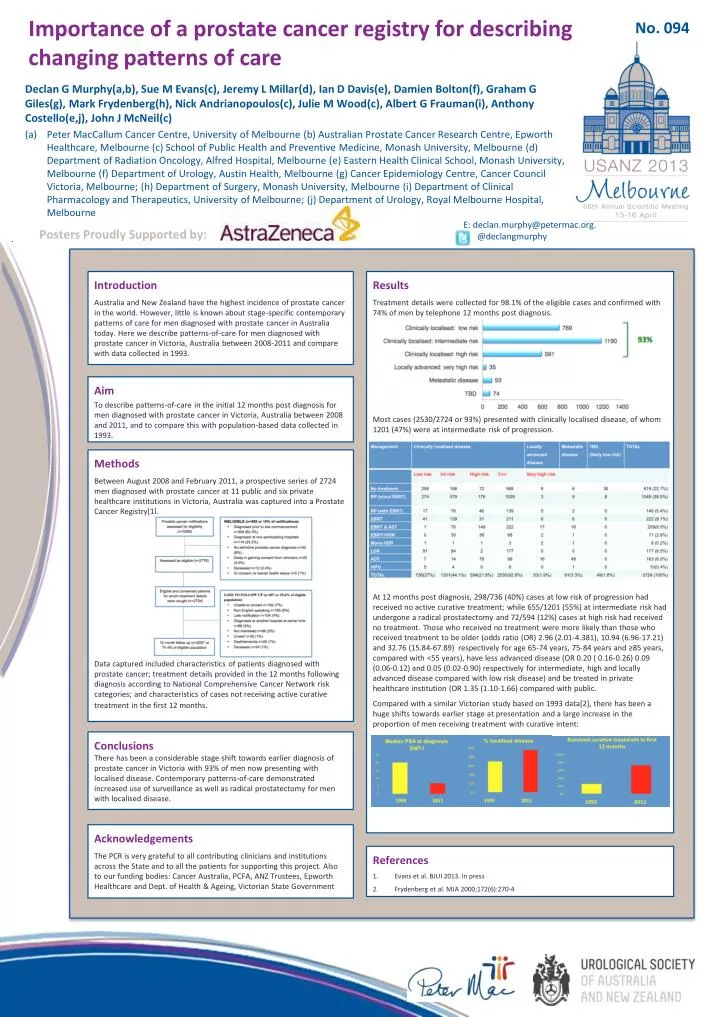
Importance of a prostate cancer registry for describing changing patterns of care No. 094 Declan G Murphy(a,b), Sue M Evans(c), Jeremy L Millar(d), Ian D Davis(e), Damien Bolton(f), Graham G Giles(g), Mark Frydenberg(h), Nick Andrianopoulos(c), Julie M Wood(c), Albert G Frauman(i), Anthony Costello(e,j), John J McNeil(c) Peter MacCallum Cancer Centre, University of Melbourne (b) Australian Prostate Cancer Research Centre, Epworth Healthcare, Melbourne (c) School of Public Health and Preventive Medicine, Monash University, Melbourne (d) Department of Radiation Oncology, Alfred Hospital, Melbourne (e) Eastern Health Clinical School, Monash University, Melbourne (f) Department of Urology, Austin Health, Melbourne (g) Cancer Epidemiology Centre, Cancer Council Victoria, Melbourne; (h) Department of Surgery, Monash University, Melbourne (i) Department of Clinical Pharmacology and Therapeutics, University of Melbourne; (j) Department of Urology, Royal Melbourne Hospital, Melbourne • E: declan.murphy@petermac.org. C @declangmurphy Posters Proudly Supported by: Results Treatment details were collected for 98.1% of the eligible cases and confirmed with 74% of men by telephone 12 months post diagnosis. Most cases (2530/2724 or 93%) presented with clinically localised disease, of whom 1201 (47%) were at intermediate risk of progression. At 12 months post diagnosis, 298/736 (40%) cases at low risk of progression had received no active curative treatment; while 655/1201 (55%) at intermediate risk had undergone a radical prostatectomy and 72/594 (12%) cases at high risk had received no treatment. Those who received no treatment were more likely than those who received treatment to be older (odds ratio (OR) 2.96 (2.01-4.381), 10.94 (6.96-17.21) and 32.76 (15.84-67.89) respectively for age 65-74 years, 75-84 years and ≥85 years, compared with <55 years), have less advanced disease (OR 0.20 ( 0.16-0.26) 0.09 (0.06-0.12) and 0.05 (0.02-0.90) respectively for intermediate, high and locally advanced disease compared with low risk disease) and be treated in private healthcare institution (OR 1.35 (1.10-1.66) compared with public. Compared with a similar Victorian study based on 1993 data[2], there has been a huge shifts towards earlier stage at presentation and a large increase in the proportion of men receiving treatment with curative intent: Introduction Australia and New Zealand have the highest incidence of prostate cancer in the world. However, little is known about stage-specific contemporary patterns of care for men diagnosed with prostate cancer in Australia today. Here we describe patterns-of-care for men diagnosed with prostate cancer in Victoria, Australia between 2008-2011 and compare with data collected in 1993. Aim To describe patterns-of-care in the initial 12 months post diagnosis for men diagnosed with prostate cancer in Victoria, Australia between 2008 and 2011, and to compare this with population-based data collected in 1993. Methods Between August 2008 and February 2011, a prospective series of 2724 men diagnosed with prostate cancer at 11 public and six private healthcare institutions in Victoria, Australia was captured into a Prostate Cancer Registry[1]. Data captured included characteristics of patients diagnosed with prostate cancer; treatment details provided in the 12 months following diagnosis according to National Comprehensive Cancer Network risk categories; and characteristics of cases not receiving active curative treatment in the first 12 months. Conclusions There has been a considerable stage shift towards earlier diagnosis of prostate cancer in Victoria with 93% of men now presenting with localised disease. Contemporary patterns-of-care demonstrated increased use of surveillance as well as radical prostatectomy for men with localised disease. Acknowledgements The PCR is very grateful to all contributing clinicians and institutions across the State and to all the patients for supporting this project. Also to our funding bodies: Cancer Australia, PCFA, ANZ Trustees, Epworth Healthcare and Dept. of Health & Ageing, Victorian State Government References Evans et al. BJUI 2013. In press Frydenberg et al. MJA 2000;172(6):270-4