Download
1 / 39
400 likes | 485 Views
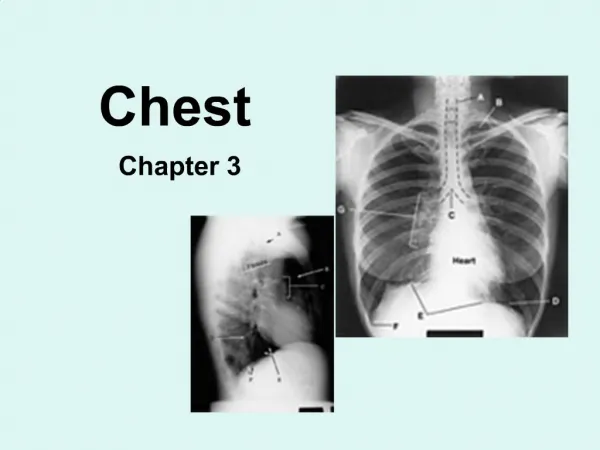
Reading Chest Radiographs. Basics. Anterior-Posterior vs. Posterior-Anterior AP exaggerates cardiac size PA requires pt to stand Look at the whole radiograph Learn a system - do it the same EVERY time. System. A-B-C-D-E-F A - Airway/lung fields B - Bones/soft tissue

E N D
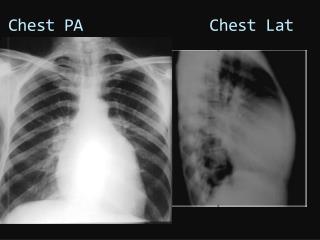
Basics • Anterior-Posterior vs. Posterior-Anterior • AP exaggerates cardiac size • PA requires pt to stand • Look at the whole radiograph • Learn a system - do it the same EVERY time
System • A-B-C-D-E-F • A - Airway/lung fields • B - Bones/soft tissue • C - Cardiac/mediastinum • D - Diaphragm • E - Examine Technique • F - Foreign bodies
Lung Parenchyma • Classify disease into 3 categories • Airspace: alveolar filling • fluffy, opacities, air-bronchograms • Interstitial: lines and small dots • reticulonodular, reticular, nodular • Nodule: single or multiple, vary in size, w/ or w/o cavitation/calcification, smooth or irregular
Consolidation • Filling or loss of air spaces • Pus - Pneumonia • Fluid - Pulmonary edema • Blood - infarct, hemorrhage • Foreign body - aspiration • Tumor - bronchoalveolar carcinoma • Volume loss - atelectasis
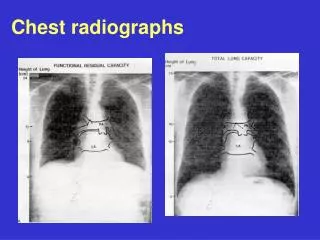
Consolidation • Radiographic signs • Opacity, air bronchograms, silhouetting • Silhouette sign: intrathoracic lesion touching border of heart, aorta, diaphragm obliterating that border • Helps to identify location of consolidation
Left Heart Silhouette sign
Consolidation • Silhouette sign: • What structure is silhouetted on PA? • R heart = RML • L heart = lingula • Aorta, diaphragm = Lower lobe • Lateral view: which diaphragm is silhouetted? • Fissure sign: abrupt edge @ margin • Increased density of vert. just above diaphragm on lateral
Collapse • Atelectasis - volume loss • Extrinsic compression (effusion, tumor, etc) • Airway obstruction • Extraluminal - tumor, LAD • Intraluminal - tumor, foreign body • Lobar collapse: mediatstinal shift to affected side, displacement of hilum/fissures, fewer vessels on affected side
Interstitial Pattern • Acute process: • Pneumonia - viral, fungal, Tb, PCP • Edema - CHF, Renal failure w/ overload • Drug/Transfusion reaction • Chronic: many etiologies • Normal/low lung volumes
Interstitial Pattern • Upper lobe predominant • Tb, pneumoconioses, fibrosis from ankylosing spondylitis • Mid lung predominant • sarcoid, berylliosis, allergic alveolitis, eosinophilic granulomatosis • Lower lung predominant • IPF, lymphangitic tumor spread, CVD fibrosis, chronic edema, drug rxn
Interstitial Pattern • Large Lung volumes: indicates air trapping • Cystic fibrosis • Eosinophilic granulomatosis • Lymhangioleiomyomatosis • Tuberous sclerosis
Pulmonary Nodule(s) • Solitary Nodule: many etiologies • Primary lung tumor, mets, granuloma, septic emboli, pulmonary AVM, hamartoma, Wegener’s vasculitis, bronchiectasis, fungal infection, etc • Important features • Change over time: growing is worrisome • Calcification: eccentric is worrisome • Size: > 3cm more worrisome
Pulmonary Nodule(s) • Multiple Nodules • Metastatic until proven otherwise • septic/bland emboli • vasculitides, CVD • pneumoconioses • Eosinophilic granulomatosis • Fungi, viral, Tb PNA • Wegener’s • Lymphoma
Cardiac Anatomy • Frontal view • Right atrium • SVC • Aortic knob • Left atrial appendage • Left ventricle Lateral view Right atrium/Ventricle Left ventricle Left atrium Aortic arch Main Pulm. Artery Descending Thoracic Aorta
Cardiac Anatomy • On frontal CXR - 45% or less than largest diameter from inner aspect of rib to rib laterally • Right heart border - mostly RA • Left Border - Aortic arch, MPA, LAA, LV
Atrial/Ventricular Hypertropy • Right Atrium - Right border >4cm from center of spine • Right Ventricle - fills retrosternal space >1/3 distance between diaphragm & sternomanubrial joint • Left Atrium - subcarinal angle >90 degrees, posterior deviation of left main stem bronchus • Left Ventricle - LV reaches spine prior to diaphragm
Pulmonary Vasculature • Many potential patterns to help narrow differential for cardiac disease • 3 you need to know • Normal - lower lobe vessels larger due to gravity, taper smoothly to periphery, interlobar arterial size (11-16mm M, 9-14mm F)
Pulmonary Vasculature • Pulmonary venous hypertension: upper lobe vessels larger “cephalization” result of hypoxic vasoconstriction; dependent edema • LV failure (ASCHD, valvular), atrial myxoma, PVOD • Pulmonary arterial hypertension: “pruning” or rapid tapering of peripheral vessels from large central arteries • Chronic venous HTN, COPD, Chronic PE, vasculitides, Primary PHTN, L-to-R shunt
Mediastinum • Several compartments • Anterior: ant. = sternum, post. = pericardium • Middle: ant. = pericardium, post. = trachea • Posterior: ant. = trachea, post. = ribs • Don’t miss a widened mediastinum = could be an aortic aneurysm
Mediastinum • Masses by compartment • Anterior: “4T’s” • Teratoma • Thymoma • Terrible tumor (lymphoma, mets) • Thyroid - goiter • Middle: • Aortic aneurysm
Mediastinum • Lymph nodes - Lymphoma/Mets • Pericardial/bronchogenic cyst • Posterior: • Aneurysm • Lymph nodes • Neurogenic tumors - ganglion tumor • Spine - osteophyte • Esophagus - paraesophageal hernia • Substernal Thyroid
Pleural Abnormalities • Effusions: fluid • 300-500cc to blunt CP angle on frontal • 150cc posterior to blunt CP angle on lateral • Free flowing or not?: obtain bilateral decubital films • Subpulmonic: lateral peaking of diaphragm, loss lung parenchyma below diaphragm
Pleural Abnormalities • Pneumothorax: air in pleural space • Apical or “deep sulcus” • Tension: flattened ipsilateral lung on mediastinum • Masses • Angle w/ chest wall is obtuse • Center of Mass • Well defined margin only on 1 side
Pleural Abnormalities • Thickening • Focal: unilateral • usually from infection/hemorrhage • Plaque from asbestosis - near • diaphragms • Diffuse: unilateral • Smooth: Old Tb, empyem, hemothorax, • mesothelioma, mets, lymphoma • Nodular: same except Tb