Download
1 / 79
790 likes | 1.06k Views
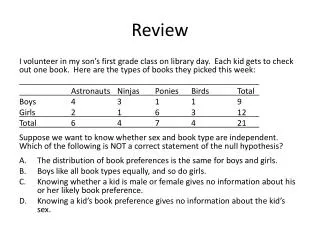
Review. Emergent/emergency/immediate phase. Assessment-History, level of consciousness, physical assessment, type of burn, burn area percentage and depth. Maintaining airway clearance Fluids replacement Support Vital sign Catheterization/insert foley catheter. Review.

E N D
Review • Emergent/emergency/immediate phase. • Assessment-History, level of consciousness, physical assessment, type of burn, burn area percentage and depth. • Maintaining airway clearance • Fluids replacement • Support Vital sign • Catheterization/insert foley catheter
Review • Blood investigation/imaging • Insert nasogastric tube
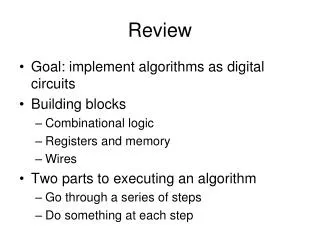
Maintaining body T° Assessment History Vital signs Intravenous line Nasogastric tube ER Pain control Indwelling catheter Neurological assessment Physical examination Emotional support Wound care
Analgesics: Pain control • Pain is more severe in second degree burns than in third degree burns because the nerve endings are not destroyed. • Exposed nerve endings are sensitive to cool, moving air. • Therefore, a sterile covering can help to reduce pain. • Measure the patient level of pain, using a consistent measurement tool. • Intravenous administered narcotics such as morphine, fentanyl are the best med for managing pain.
Analgesics: Pain control • Large doses are avoided because of the danger of respiratory depression • Subcutaneous or intramuscular routes are not recommended-↓impaired circulation in the injured tissue. • Symptoms of restlessness and anxiety, often attributed to pain. • Patient controlled analgesia(PCA) enhances the patient ability to cope with pain. .
Maintaining body temperature • The environment must be heat controlled and kept warmer than usual. • Room temperature is maintained at 22°C to24°C with humidity of 40%-50%. • Heat lamps and warming blankets are used during burn shock. • Prolonged exposure to air is avoided. • Wound covered with sterile sheets.
Providing initial wound care • Care of the burn wound can be delayed until first aid measures have been initiated. • The goal: 1.Cleanse the wound to eliminate or decrease the dead tissue and debris that serve as the media for bacterial growth. 2. Prevent further destruction of viable skin. 3. Provide for patient comfort.
Providing initial wound care • During the admission procedure-wound and the entire body are washed to removed dirt and debris. • Gentle cleansing with gauze is effective in removing dead tissue. • All hair in and around the burn wound is shaved and wiped off the skin because hair attracts bacteria. • Intact blisters may remain undisturbed because they are natural protective and pain-free dressing. • If the blisters are broken and the epidermis is separated, the wound must be clean.
Providing initial wound care • Before a dressing is applied, cultures of the wound are obtained • Baseline cultures provide information about organisms present. • Photographs are taken on admission and at intervals during the patient hospitalization. Providing comfort • Kept comfortable as possible by gentle handling of the burn areas and by keeping the wounds covered so that air does reach them.
Providing emotional support • May experience profound insult to their body and self-image. • Fear and helplessness because the victim aware that they may not survive. • Unknown surroundings and people-emotional stress. Intervention to ↓anxiety • identify self to the patient
Intervention to ↓anxiety • Orient the patient to the surroundings • Describe the basis for physical symptoms (skin loss, pain, and cold) • Explain the equipment and procedures to be used in treatment.
Maintaining body T° Assessment History Vital signs Intravenous line Nasogastric tube ER Pain control Indwelling catheter Neurological assessment Physical examination Emotional support Wound care
ACUTE PHASE Other medication Nutrition Wound Cleansing and debridement Relieving anxiety
Acute phase • Begins at the end of the emergent phase and lasts until the burn wound is heal. • Length of this period is about 7 to 21 days. • If the burn is full-thickness/large % acute phase last for months. Focus of management:- 1.Treatment of the burn wound. 2.Avoidance, detection and treatment of complication.
Other medication • Analgesics • Antiemetics • Sedatives • H2 antagonists • Antibiotics – not used for routine prophylaxis, reserved for invasive infection • Blood transfusion – for severe burns and forsurgery
Medication Tetanus Immunization For tetanus prophylaxis, tetanus toxoid 0.5 ml should be provided unless the patient has received tetanus immunization within the past 5 years. Vitamins • There are no formal rules provide vitamin and trace element supplementation in burn patients. • Most recommendations are based on observations of burn wound nutrient losses.
Vitamins Vitamin C • Vitamin C is an essential co-factor in the hydrolysis in collagen biosynthesis. • Lack of vitamin C causes capillary fragility and wound breakdown. Vitamin A Vitamin A stimulates and enhances collagen accumulation in wounds
Vitamins Thiamin/vit B1 • Thiamin is necessary function in the formation of collagen. Folic Acid • Folic acid is a substrate in reactions of DNA and RNA synthesis. Inadequate vitamin B12 levels prevent folic acid utilization.
Vitamins Zinc • The hypermetabolism induced by the burn state causes excretion of zinc at a rate five times normal(nitrogen excretion in urine) • Zinc is needed for wound healing and has a key role in immune function. • Reduced zinc levels cause decreased wound epithelialization and collagen strength. • Receive supplementation of up to 220mg/day.
Vitamins Iron • Inflammation causes a decrease in intestinal iron absorption, a decreases in iron release from parenchymal storage sites, and an increase in ferritin. • These factors lead to low serum iron concentrations after injury or infection. • Low iron levels also impair the immune response.
Ulcer Prophylaxis • Burn patients are prone to peptic ulceration 1.The cause of stress ulceration is, -increased acid, bile reflux, and direct mucosal injury from intraluminal tubes. • Ulcers occur most frequently in septic patients and those with large burns • Ulcer perforation occurs in 12% of patients, but only 1/3 of these patients will feel pain or discomfort. • early antacid therapy, and early enteral feeding have become standard in the treatment of the burn patient, the incidence of clinical gastroduodenal disease decreased to less than 2%.
Ulcer Prophylaxis B. Prevention of stress ulceration involves acid reduction and aggressive fluid resuscitation to minimize mucosal ischemia. -The early institution of enteral feedings after a burn will provide acid buffering and nutrition. -Antacids, histamine-2-receptor (H2) antagonists, are considered equally effective in preventing stress ulcer-related GI bleeding, e.g famotiden/zantac IV.
Nutrition: Metabolic demand • Metabolism can be increased by 2 or 3 times because of stress, fluid loss and immobility. • Catecholamine release appears to be the major mediator of the hypermetabolic respond to burn injury. • Healing a large surface area requires much energy; glucose is the primary metabolic fuel.
Nutrition: Metabolic demand • Total body glucose stores are limited, and stored liver and muscle glycogen is exhausted within the first few days • Therefore body need nutritional support in the form of enteral/total parental nutrition may be necessary. • The adult patient may require 3,000-5,000 calorie or more per day.
Nutrition: Metabolic demand • A burn or less than 10% usually requires minimal supplementation. • A high protein, high calorie diet is necessary for a 10% to 20% burn. • Between 20% to 30%, enteral feedings are generally necessary. • The metabolic rates of patients with burns greater then 40% TBSA are 100-150% greater than their basal metabolic rate.
Nutrition: Metabolic demand • Enteral feedings given within the first 24 hours postburn:- -decrease hyper-metabolism, --improve nitrogen balance, -maintain gut mucosal integrity,
Nutrition: Metabolic demand • Enteral feedings have been shown to increase intestinal blood flow. • Total parental nutrition is generally reserved for patients who are unable to tolerate enteral feeding. • Food by mouth with supplements, such as milk or ensure, and tube feedings may be necessary to meet the patients nutritional requirements.
Nutrition: Metabolic demand • Protein needs of the burn patient are increased, due to the loss of nitrogen through burn wound exudates, in addition to urinary nitrogen losses. • Protein Need= 20% of total kilocalories
Nutrition: Metabolic demand • Smaller burns (<25% TBSA) with no associated facial injuries or inhalational injury. • receive a high protein/ high calorie diet -dietitian. Pediatric Requirements 1. Children have an increased surface area to weight ratio, greater caloric requirements than adults. 2. Protein needs in children are 11-15% of total kilocalorie requirements.
Nutrition:Tubefeeding • Patients with larger surface area burns are usually unable to meet their nutritional requirements by the oral route only. • Therefore, these patients should receive continuous tube feedings. • A nasogastric (NG) tube is first passed upon admission • Feedings are started at full strength at 20 cc/hr and increased slowly (by 10 cc/4 hrs) or rapidly (by 20 cc/4hrs) as tolerated until the goal hourly rate is achieved.
Nutrition:Tube feeding • Tube feedings are weaned as the patient increases oral intake. • tube feedings may be administered during the night time only to stimulate appetite and increase daytime oral intake. • When the patient can eat 80-90% of his caloric needs, tube feedings may be discontinued.
Relieving anxiety • During acute phase, • Patient becomes aware of extent of the injury and begin to evaluate its implications for his or her life. • Many problems may happen • A variety behavior can be seen, ↓interaction, denial, anger, depression and anxiety.
Relieving anxiety • On going education is imperative to assist the patient understanding. • It is important for the patient to maintain a sense of hope for future. • Without hope, the patient has less ability to cope and show sense of failure. • Ongoing education to assist the patient in understanding the care given and to make relistic plans for the future.
3.Excision & grafting 3a) Biological dressings 1.Cleaning & debridement General wound care 2.Antimicrobial Agents 3b) Biosynthetic & Synthetic dressing
Goals of wound care Caregivers wear gowns, masks, eye protection and gloves • Prevention of infection • Removal of devitalized tissue • Prevention of further destruction of healthy tissue. • Minimize of pain.
Wound cleansing:- debridment • Debridement removes dead tissue and blisters to expose the true depth and severity of a wound. • In some burn injuries, dead tissue naturally falls off as part of the healing process. • Some need to assist in the removal of the damaged skin. • Debridement is often an extremely painful procedure.
There are four primary methods of debridement. • Autolytic-allowing the body to naturally rid itself of dead tissue • Enzymatic-using chemical enzymes(Elase) to free dead tissue from the wound bed. • Mechanical-removing dead tissue through the use of hydrotherapy (water) -manual removal of eschar using gauze, sponges, tweezers, scissors or other instruments is performed.
There are four primary methods of debridement. • Surgical-using sharp instruments or lasers for debridement. -Surgical debridement involves cutting the dead tissue away. -Performed in the operating room with the patient under anesthesia.
Wound cleansing-Mechanical • Treatment of the burn wound includes daily or twice-daily wound cleansing or hydrotherapy (tubbing), and dressing changes. • Hydrotherpay(tubbing)-is the bathing of the burn patient in a tub of water or with a water shower to facilitate cleansing and debridement of the burned area
Hydrotherapy:advantages • Topical medications, adherent dressings, and eschar are more easily removed. • Provides an opportunity for the patient to practice range of-motion excercises. • Total assessment of the burn area is facilitated; total body cleansing can be achieved.
Hydrotherapy:disadvantages • Loss of body heat; loss of sodium • Uncomfortable and at times painful for the patient • Maintenance of intravenous lines and ventilator care may be difficult during hydrotherapy. • The patient`s anxiety level ↑, -fear of drowning -discomfort of the experience
Intervention • Describe the procedure to the patient who is experiencing hydrotherapy for the first time. • Select the time for future tubbing appropriately and administer a pain-control medication. • If patient has a indwelling catheter, drain and plug it or maintain a closed system to avoid contamination.
Methods of wound treatment • Methods of treating depending on the:- -Location of the burn, its size and depth. -Inpatient or outpatient care. -Patient`s respond to therapy. • Wounds can be managed by an open or closed method. • Open method, -allows wounds to be visualized
Methods of wound treatment Open method -more readily and assists in range of motion because of the absence of constricting dressing. Disadvantages -heat loss -easy accidental removal of the topical agent during patient activity.
Methods of wound treatment • Closed method • Topical agent is placed on the wound. • The wound is covered with gauze. • This method promotes adherence of the topical agent to the wound • Limit fluid loss and wound drying.
Dressing changes • In patient`s room. • Hydrotherapy room • Treatment area . 20 Minutes After pain killer
Antimicrobial agents • Systemic antibiotics are rarely able to reach areas of avascular eschar. • Topically applied antimicrobials provide high concentrations of antibiotic on the wound surface, where microbial numbers are the highest. • Topical antimicrobial therapy delays and minimizes wound microbial colonization