Download
1 / 18
180 likes | 332 Views
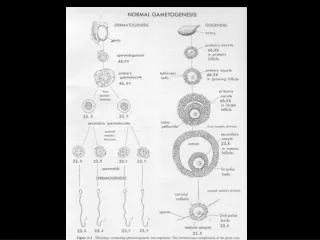
DISEASES AFFECTING TUBULES AND INTERSTITIUM . Tubulointerstitial Nephritis. Causes : 1- bacterial infection. 2- drugs. 3- metabolic disorders such as hypokalemia . 4- physical injury such as irradiation. 5- viral infections. 6- immune reactions . TIN is divided into : 1-acute

E N D
Tubulointerstitial Nephritis • Causes : • 1- bacterial infection. • 2- drugs. • 3- metabolic disorders such as hypokalemia. • 4- physical injury such as irradiation. • 5- viral infections. • 6- immune reactions. • TIN is divided into : • 1-acute • 2-chronic
Acute Pyelonephritis • a common suppurative inflammation of the kidney and the renal pelvis. • bacterial infection. • important manifestation of (UTI) : 1- lower UT (cystitis, prostatitis, urethritis). 2- upper UT(pyelonephritis). 3- both.
Pathogenesis • The principal causative organisms are : 1- Escherichia coli>is the most common . 2- Proteus. 3- Klebsiella. 4- Enterobacter. 5- Pseudomonas. 6- Staphylococci and Streptococcus faecalis (uncommon). Routes of infection • 1-hematogenous (seeding of the kidneys by bacteria in septicemia or infective endocarditis) • 2-ascending infection (most common): from the lower urinary tract
bladder urine is sterile and remains so as a result of: • 1- the antimicrobial properties of the bladder mucosa. • 2- the flushing action associated with periodic voiding of urine. • The first step is adhesion of bacteria to mucosal surfaces → colonization of the distal urethra → bladder by expansive growth of the colonies and by moving against the flow of urine. • Predisposing factors • 1-urethral instrumentation, including catheterization and cystoscopy • 2-female sex because of the close proximity of the urethra to the rectum • 3-trauma to the urethra • 4-outflow obstruction or bladder dysfunction (benign prostatic hyperplasia; uterine prolapse; neurogenic bladder dysfunction
5-Pregnancy. • 4% to 6% of pregnant women develop bacteriuria sometime during pregnancy and 20% -40% of these eventually develop UTI. • 6-UTI is increased in diabetes because of the increased susceptibility to infection. • 7-vesicoureteral reflux An incompetent vesicoureteral orifice allows the reflux of bladder urine into the ureters &allows bacteria to ascend the ureter into the pelvis. - present in 20% to 40% of young children with UTI 1- congenital defect that results in incompetence of the ureterovesical valve. 2-acquired in spinal cord injury and with neurogenic bladder dysfunction secondary to diabetes
Acute pyelonephritis. The cortical surface is studded with focal pale abscesses
Drug-Induced Interstitial Nephritis • Two forms of TIN caused by drugs are : • 1-Acute Drug-Induced Interstitial Nephritis • 2-Analgesic Nephropathy • Acute TIN • 1-most frequently occurs with synthetic penicillins (methicillin, ampicillin) • 2- other synthetic antibiotics (rifampin), diuretics (thiazides) • 3- nonsteroidal anti-inflammatory agents • 4-other drugs (phenindione, cimetidine
Pathogenesis • Many features of the disease suggest an immune mechanism. • Clinical evidence of hypersensitivity is not dose related. • Serum IgE levels are increased in some persons suggesting type I hypersensitivity. • The mononuclear or granulomatous infiltrate, together with positive skin tests to drugs, suggests a T cell-mediated (type IV) hypersensitivity reaction.
Morphology • the interstitium shows pronounced edema and infiltration by mononuclear cells, lymphocytes and macrophages . • Eosinophils and neutrophils may be present, often in large numbers. • With some drugs (e.g., methicillin, thiazides, rifampin), interstitial non-necrotizing granulomas with giant cells may be seen. • The glomeruli are normal except in some cases caused by nonsteroidal anti-inflammatory agents.
Clinicalcourse • The disease begins about 15 days (range 2-40 days) after exposure to the drug. • It is characterized by fever, eosinophilia & rash in about 25% of persons, and renal abnormalities. • Renal findings include hematuria, minimal or no proteinuria, and leukocyturia (sometimes including eosinophils). • A rising serum creatinine or acute renal failure with oliguria develops in about 50% of cases, particularly in older patients. • It is important to recognize drug-induced renal failure, because withdrawal of the offending drug is followed by recovery although it may take several months for renal function to return to normal
Analgesic Nephropathy • Consumption large quantities of analgesics may cause chronic interstitial nephritisoften associated with renal papillary necrosis. • Although at times ingestion of single types of analgesics has been incriminated, most people who develop this nephropathy consume mixtures containing some combination of phenacetin, aspirin, acetaminophen, caffeine, and codeine for long periods. • Aspirin and acetaminophen • While they can cause renal disease in apparently healthy individuals preexisting renal disease seems to be a necessary precursor to analgesic-induced renal failure
Pathogenesis • not entirely clear. • Papillary necrosis is the initial event, and the interstitial nephritis in the overlying renal parenchyma is a secondary phenomenon. • covalent binding and oxidative damage Acetaminophen • inhibition of prostaglandin synthesisaspirin • Morphology • The papillae show coagulative necrosis • dystrophic calcification may occur in the necrotic areas. • tubular atrophy, interstitial scarring, and inflammation. • The small vessels in the papillae and urinary tract submucosa exhibit characteristic PAS-positive basement membrane thickening.
Clinical Course • Chronic renal failure, hypertension, and anemia. • The anemia results in part from damage to red cells by phenacetin metabolites. • A complication of analgesic abuse is the increased incidence of transitional-cell carcinoma of the renal pelvis or bladder in persons who survive the renal failure.
Acute Tubular Necrosis (ATN) • ATN is a clinicopathologic entity characterized morphologically by damaged tubular epithelial cells and clinically by acute suppression of renal function. • It is the most common cause of acute renal failure. • In acute renal failure, urine flow falls within 24 hours to less than 400 mL/day (oliguria). • Other causes of acute renal failure include : (1) severe glomerular diseases manifesting as RPGN. (2) diffuse renal vascular diseases such as microscopic polyangiitis and thrombotic microangiopathies. (3) acute papillary necrosis associated with acute pyelonephritis. (4) acute drug-induced interstitial nephritis. (5) diffuse cortical necrosis
ATN is a reversible renal lesion. • predisposing clinical settings: • ischemic ATN is associated with shock • 1- severe trauma. • 2- acute pancreatitis. • 3- septicemia. • 4- mismatched blood transfusions and other hemolytic crises, as well as myoglobinuria. • nephrotoxic ATN • poisons including heavy metals (e.g., mercury) • organic solvents (e.g., carbon tetrachloride) • drugs such as gentamicin and other antibiotics, and radiographic contrast agents.
Pathogenesis (1) tubular injury (2) persistent and severe disturbances in blood flow resulting in diminished oxygen and substrate delivery to tubular cells. • Tubular epithelial cells are particularly sensitive to anoxia and are also vulnerable to toxins. • Ischemia causes numerous structural alterations in epithelial cells • Loss of cell polarity reversible early event. • Redistribution of membrane proteins (e.g., Na+, [Kgr ]+-ATPase) from the basolateral to the luminal surface of tubular cells • Decreased sodium reabsorption by proximal tubules and hence increased sodium delivery to distal tubules. • Vasoconstriction. • Redistribution or alteration of integrins that anchor tubular cells to their underlying basement membranes results in shedding of tubular cells into the urine