Download
1 / 2
60 likes | 262 Views
Adolescent Polycystic Ovary Syndrome (PCOS) is a Precursor of Adult PCOS and Glucose Intolerance B.D. Bordini, E.E. Baumann, and R.L Rosenfield Section of Pediatric Endocrinology. Abstract. Results. Summary. PCOS and Endocrinologic Heterogeneity

E N D
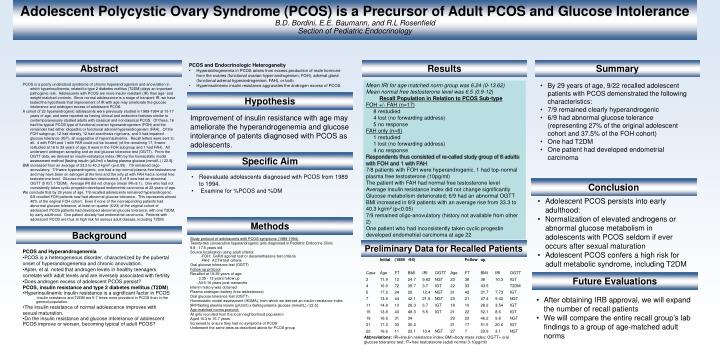
Adolescent Polycystic Ovary Syndrome (PCOS) is a Precursor of Adult PCOS and Glucose Intolerance B.D. Bordini, E.E. Baumann, and R.L RosenfieldSection of Pediatric Endocrinology Abstract Results Summary • PCOS and Endocrinologic Heterogeneity • Hyperandrogenemia in PCOS arises from excess production of male hormone from the ovaries (functional ovarian hyper-androgenism, FOH), adrenal gland (functional adrenal hyperandrogenism, FAH), or both. • Hyperinsulinemic insulin resistance aggravates the androgen excess of PCOS. • By 29 years of age, 9/22 recalled adolescent patients with PCOS demonstrated the following characteristics: • 7/9 remained clearly hyperandrogenic • 6/9 had abnormal glucose tolerance (representing 27% of the original adolescent cohort and 37.5% of the FOH cohort) • One had T2DM • One patient had developed endometrial carcinoma PCOS is a poorly understood syndrome of chronic hyperandrogenism and anovulation in which hyperinsulinemia, related to type 2 diabetes mellitus (T2DM) plays an important pathogenic role. Adolescents with PCOS are more insulin resistant (IR) than age- and weight-matched controls. Since normal adolescence is a stage of transient IR, we have tested the hypothesis that improvement of IR with age may ameliorate the glucose intolerance and androgen excess of adolescent PCOS. A cohort of 23 hyperandrogenic adolescents were previously studied in 1989-1994 at 10-17 years of age, and were reported as having clinical and endocrine features similar to contemporaneously studied adults with classical and nonclassical PCOS. Of these, 16 had the typical PCOS type of functional ovarian hyperandrogenism (FOH) and the remainder had either idiopathic or functional adrenal hyperandrogenism (FAH). Of the FOH subgroup, 12 had obesity, 12 had acanthosis nigricans, and 3 had impaired glucose tolerance (IGT), all suggestive of hyperinsulinemia. Recall letters were sent to all. 4 with FOH and 1 with FAH could not be located; (of the remaining 17, 9 were restudied at 18 to 29 years of age; 8 were in the FOH subgroup and 1 had FAH). All underwent androgen sampling and an oral glucose tolerance test (OGTT). From the OGTT data, we derived an insulin-resistance index (IRI) by the homeostatic model assessment method [fasting insulin (μIU/ml) x fasting plasma glucose (mmol/L) / 22.5]. BMI increased from an average of 33.2 to 40.3 kg/m2 (p<0.05). 7/9 remained oligo-anovulatory. 7/9 were hyperandrogenic, one had a top-normal plasma free testosterone and may have been on estrogen at the time and the only pt with FAH had a normal free testosterone level. Glucose metabolism deteriorated, 6 of 9 now had an abnormal OGTT (5 IGT, 1T2DM). Average IRI did not change (mean IRI=9.1). One who had not consistently taken cyclic progestin developed endometrial carcinoma at 22 years of age. We conclude that by 29 years of age, 7/9 recalled adolescents remained hyperandrogenic. 6/8 recalled FOH patients now had abnormal glucose tolerance. This represents almost 40% of the original FOH cohort. Even if none of the nonresponding patients had abnormal glucose tolerance, at least on quarter (6/23) of the original cohort of adolescent PCOS patients had developed abnormal glucose tolerance, with one T2DM, by early adulthood. One patient already had endometrial carcinoma. Patients with adolescent PCOS are thus at high risk for serious adult disease, including T2DM. • Mean IRI for age matched norm group was 6.24 (0-13.62) • Mean normal free testosterone level was 6.5 (0.9-12) • Recall Population in Relation to PCOS Sub-type • FOH +/- FAH (n=17) • 8 restudied • 4 lost (no forwarding address) • 5 no response • FAH only (n=6) • 1 restudied • 1 lost (no forwarding address) • 4 no response • Respondents thus consisted of re-called study group of 8 adults with FOH and 1 with FAH • 7/8 patients with FOH were hyperandrogenic, 1 had top-normal plasma free testosterone (10pg/ml) • The patient with FAH had normal free testosterone level • Average insulin resistance index did not change significantly • Glucose metabolism deteriorated; 6/9 had an abnormal OGTT • BMI increased in 8/9 patients with an average rise from 33.3 to 40.3 kg/m2 (p<0.05) • 7/9 remained oligo-anovulatory (history not available from other 2) • One patient who had inconsistently taken cyclic progestin developed endometrial carcinoma at age 22 Hypothesis Improvement of insulin resistance with age may ameliorate the hyperandrogenemia and glucose intolerance of patents diagnosed with PCOS as adolescents. Specific Aim • Reevaluate adolescents diagnosed with PCOS from 1989 to 1994. • Examine for %PCOS and %DM Conclusion • Adolescent PCOS persists into early adulthood: • Normalization of elevated androgens or abnormal glucose metabolism in adolescents with PCOS seldom if ever occurs after sexual maturation • Adolescent PCOS confers a high risk for adult metabolic syndrome, including T2DM Methods Background Study protocol of adolescents with PCOS symptoms (1989-1994) Twenty-two consecutive hyperandrogenic girls diagnosed in Pediatric Endocrine Clinic 9.9 - 17.5 years old Source localization using adult criteria: -FOH: GnRH agonist test or dexamethasone test critieria -FAH: ACTH test criteria Oral glucose tolerance test (OGTT) Follow up protocol Recalled at 18-29 years of age: - 3.35 - 13 years follow up - All 6-16 years post-menarche Interim history was obtained Plasma androgen battery (free testosterone) Oral glucose tolerance test (OGTT) Homeostatic model assessment (HOMA), from which we derived an insulin-resistance index [IRI=fasting plasma insulin (μIU/ml) x fasting plasma glucose (mmol/L) / 22.5] Age-matched norms protocol: All girls recruited from the local neighborhood population Aged 10.3 to 16.7 years Screened to ensure they had no symptoms of PCOS Underwent the same tests as described above for PCOS group Preliminary Data for Recalled Patients • PCOS and Hyperandrogenemia • PCOS is a heterogeneous disorder, characterized by the pubertal onset of hyperandrogenemia and chronic anovulation. • Apter, et al. noted that androgen levels in healthy teenagers correlate with adult levels and are inversely associated with fertility • Does androgen excess of adolescent PCOS persist? • PCOS, insulin resistance and type 2 diabetes mellitus (T2DM) • Hyperinsulinemic insulin resistance is a significant factor in PCOS • -Insulin resistance and T2DM are 5-7 times more prevalent in PCOS than in the general population. • The insulin resistance of normal adolescence improves with sexual maturation. • Do the insulin resistance and glucose intolerance of adolescent PCOS improve or worsen, becoming typical of adult PCOS? Future Evaluations • After obtaining IRB approval, we will expand the number of recall patients • We will compare the entire recall group’s lab findings to a group of age-matched adult norms
Molecular Basis of Hormone Deficiency J. Curley, E. Rochowicz-Wirthwein, J. Robbins, mentor - S. Radovick University of Chicago Children’s Hospital Prop-1 Gene A -> T (nt 343) 5’ 3’ Rathke's Deficient Factor Prop-1 ACTH def. Primer Sequence GH def. LH/FSH def. PRL def. TSH def. Pouch R73C R73H S109X F117I P164X S83P F88S P160X R99X R99Q Exon #1 sense 5’-GGAAGCAGAGAAATCTCAAGTC-3’ antisense 5’-AAAGCCAAGGGGTGCTCCAGTC-3’ Rpx Yes Yes Yes Yes Yes R120C Ptx-2 No Yes Yes Yes Yes Exon #2 sense 5’-TGGTCCAGCACCGAGGAGCGTC-3’ antisense 5’-TAATGCCCAACATTCTATGATAGC-3’ Lhx-3 No Yes Yes Yes Yes GH PRL ACTH LH / FSH TSH Exon #3 sense 5’-GTGTCACCACCTATGTCAAGTGTG-3’ antisense 5’-TCCTAATCGGTGAGCTGACCCTCA-3’ Prop-1 No Yes +/- Yes Yes Pit-1 No Yes No Yes Yes Introduction Methods Methods - cont. Results - cont. Conclusion Pituitary development and hormone expression in mammals is controlled by pituitary-specific transcription factors including Hesx-1 (Rpx), Ptx-2, Lhx-3, Prop-1, and Pit-1. These factors initiate a cascade of development events resulting in mature pituitary cell-types, and a mutation or deletion of the genes encoding these factors has been shown to result in anterior pituitary hormone deficiency in mammals. FIGURE 1. Overview of anterior pituitary development.d Mutations in these genes encoding pituitary-specific transcription factors contribute to the growth hormone deficient phenotype (i.e. short stature) +/- other pituitary hormone deficiency phenotypes by interrupting the cascade of development and maturation of the pituitary-cell types and thus, cause hormone deficiency(ies) (GH +/- ACTH, LH/FSH, TSH, and PRL) in these patients. TABLE 1. Hormone deficiencies associated with the transcription factors investigated in this work. The goal of this work was two-fold. First, to identify novel mutations in these candidate genes encoding pituitary-specific transcription factors in a pituitary-hormone deficient patient. Second, to determine the mechanism by which any mutation causes hypopituitarism. • Direct Sequencing: 5 uL PCR product, 1 uL primer (sense OR antisense), and 4 uL ABI prism sequencing solution.Then, sequence reaction on PCR machine. Finally, purify: • 2 uL 3 M NaAc+50 uL 95% EtOH-vortex, ice x10”, cold centrifuge x 20”, decant supernatant, add 250 uL 70% EtOH + cold centrifuge x 5”, decant supernatant, dry pellet • Indirect sequencing: • Ligation: Ligate PCR product into pTOPO with ECOR1 on each side: 1 uL TOPO vector, 1 uL PCR product, 1 uL salt solution, and 1 uL H2O: incubate 30 min at room temperature • Transformation: 100 uL thawed DH5- cells + 3 uL Ligation mix, then ice x 15”; to ‘shock,’ incubate @ 37° x 45 sec then return to ice x 2”; 900 uL LB – shaker X 1’; 100 ul IPTG + xGAL; culture plates (w/ Amp)- 37° overnight; 3 mL Circle Grow(+Amp) + white colony; Shaker overnight • Miniprep yields DNA then mix 4 uL with 4 uL H2O, 1 uL buffer H, 1 uL ECOR1and leave 1 hour at 37° • Sequencing reaction with T7 solution • Compare Sequences to published exon sequences (NCBI Sequence viewer-website) and wild type sequences. • I. PATIENT XX, PHENOTYPE • Blood obtained from patient who was an ex 34 week infant of nonconsanguinous parents. In his neonatal period he had hypoglycemia, seizures, micropenis, and prolonged indirect hyperbilirubinemia. He had the following evaluation: • cortisol 1.54 mcg/dl • on ACTH stim test, basal cortisol was 3.6 mcg/dl and at 6 hrs was 3.44 mcg/dl. • LH/FSH - no information • TSH 0.07 mIU/ml (0.35-5.5) • PRL 36 ng/dl (12-27) • OPTIC NERVE - no information • XX was started on hydrocortisone, Na thyroxine, and synthetic growth hormone therapy. • II. CANDIDATE GENES PROBED • Genomic DNA made w/Qiagen Flexigene DNA Kit • PCR conditions optimized for each exon • i.e. buffers, MgCl2 • Invitrogen Optimizer Settingwith variedannealing temperatures • Individual or consecutive exons of candidate genes amplified by PCR (Table 2). • TABLE 2. Primers used in PCR of Prop-1. • PCR products cleaned with Exo-Sap-IT to eliminate primers, primer-dimers, and nucleotides before sending for sequencing: 5 uL Shrimp Alkaline Phosphatase (SAP) Buffer; 0.5 uL SAP; 0.5 uL E. coli Exonuclease I;37° x 45”,95° x 15”, store at 4° • Exons directly or indirectly sequenced (next column) at a DNA sequencing facility. R50D Del 112-114 FIGURE 5. Known mutations in the paired-like homeodomain transcription factor Prop-1 (prophet of Pit-1).d A142T lies just outside of the homeodomain (black shading) of Prop-1 in exon 3. This would be near a conserved basic region, B2, required for nuclear localization, DNA binding, and target gene activation. Other possible effects could include transcription modification via changed tertiary structure. A142T is noted to be a possible polymorphism. Given geographical association of this reported polymorphism,a the substitution could be a mutation with a discernable change in function. Accordingly, transfection assays are underway to combine with a luciferase reporter system and probe function quantitatively, and initial results are promising. Parental samples have been obtained for analysis. Limitations of this work include incomplete patient description as well as other candidate genes which are not yet assayed. Rpx Pitx a-GSU Lhx3/Lhx4 FIGURE 3. Rpx 1 exon 4 is wild type in patient XX. The PCR products (i.e. from gel such as in Figure 2) were sequenced and compared to the published exon sequences. Shown here is an assembling and confirmation that XX has the wild type sequence for part of RPX1 exon 4 (confirmed throughout sequence). Table 3. Of the sequences optimized and analyzed, a possible mutation in Prop-1 was found. DNA-binding tested in gel shift assays utilizing radiolabeled consensus DNA-binding elements and protein translated in reticulocyte lysate to assess the ability of wild type and mutant proteins to bind to known response elements. A typical TNT T7 kit recipe follows: 40 L lysate, 1.5 mcg DNA, 1 L met, 7.5 L water, mix, spin, 30o x 1-2 hrs, spin. Probe was 15 L DIDC, 1.5 L 0.1 M DTT, 2 L PRDQ9 probe P-32, 130 L BSB buffer. Lanes 1 and 2 were loaded with 4 L lysate mixture and 10 L probe. Prop-1 Pit-1 (Prop-1) SF-1 GATA2 NeuroD1 GATA2 rostral caudal lactotroph gonadotroph thyrotroph somatotroph corticotroph Results 1 2 3 4 5 6 7 8 9 10 Support/IRB information <-- a <-- b <-- c FIGURE 2. Optimizing PCR conditions to obtain introns of two transcription factors, Rpx1 and Ptx-2; success at ~700 Bp for Ptx-2 exon 7 (band b) in this gel. Band a is DNA in the well, and band c is Rpx primer-dimer. Lanes 1-2 are HI-LO standard (Bionexus); lanes 3-6 are Rpx exon 3 sense and exon 4 antisense primers at 60o, buffer M; lanes 7-10 are Ptx-2 exon 7 sense and antisense, standard buffer, 60o. PCR reaction sample preparation:40 L H2O, 1 L primer (sense), 1 L primer (anti-sense), 5 L buffer, 4 L d NTP, 1 L DNA, and 0.5 L TAQ Polymerase. RO1 DK 53977 Differential Regulation of Pit-1 Responsive Genes by CBP K24 DK 01362 Hypopituitarism: clinical and molecular characterization IRB Approval 2/5/02; IRB Protocol # 10838B Figure 4.WT Prop-1 and A142T bind target DNA to approximately the same extent. In lane 1 WT Prop-1, while lane 2 has the potential mutation, A142T. Control lane with empty vector is not shown but revealed no shift. 1 2 References aNakamura, Y., Usui, T., Mizuta, H., Murabe, H., Muro, S., Suda, M., Tanaka, K., Tanaka, I., Shimatsu, A, and Nakao, K. Characterization of Prophet of Pit-1 gene expressioin in normal pituitary and pituitary adenomas in humans. J. Clin. Endocrinology & Met.; 1999; 84(6): 1414. bVallette-Kasie, S., Barlier, A., Teinturier, C., Diaz, A., Manavela, M., Berthezene, F., Bouchard, P., Chaussain, J. L., Brauner, R., Pellegrini-Bouiller, I., Jaquet, P., Enjalbert, A., Brue, T. Prop1 Gene screening in patients with multiple pituitary hormone deficiency reveals two sites of hypermutability and a high incidence of corticotroph deficiency. JCEM; 2001: 86(9): 4529. cGuy, J. C., Hunter, C. S., Showalter, A.D., Smith, T. P. L., Charoonpatrapong, K., Sloop, K.W., Bidwell, J. P., Rhodes, S. J. Conserved amino acid sequences confer nuclear localization upon the prophet of Pit-1 pituitary transcription factor protein: Gene: 2004; 336, 263. dCohen, L.E., Radovick, S. Other transcription factors and hypopituitarism. Reviews in Endo. & Metobolic Disorders, 2002; 3; 301-311.