Download
1 / 39
480 likes | 1.06k Views
Polycystic ovarian syndrome. Prof. Yousef Gadmour Al- Fateh university Al- Jalla Maternity Hospital Tripoli - Libya. Polycystic ovarian syndrome. Definition :

E N D
Polycystic ovarian syndrome Prof. Yousef Gadmour Al- Fateh university Al- Jalla Maternity Hospital Tripoli - Libya
Polycystic ovarian syndrome Definition : It is a clinical syndrome characterized by presence of polycystic ovary and symptoms such as : 1. Infertility . 2. Hirsutism. 3. Oligo-amenorrhoea. 4. Obesity. 5. Dysfunctional uterine bleeding. 6. Verilisation. 7. Hyperprolactinaemia.
Incidence - It is the Commonest endocrinal gynecologic disorder -About 2% of general population. - 4-10% based on clinical, biochemical and u/s criteria. - 10-20% based on U/s only. - 30% of infertility. - 90% of Hirsutism with regular cycle. - 87% of case of oligomenorrhea. - 82% of cases with recurrent miscarriage.
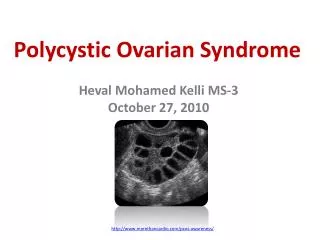
Pathology: The ovaries are enlarged and show : • Numerous small cystic follicles ( usually 2-8 mm in diameter and peripherally placed ) . • Thickened white ovarian capsule . • Theca cell hyperplasia ( due to increased LH ). • Granulosa cell atresia ( due to low FSH ) . The cystic follicles and increased ovarian stroma can be demonstrated by ultrasound .
Endocrine abnormalities : ( cont.) • Androgens – ovarian androgens excretion (testosterone and androstenedione )is commonly increased but the adrenal (dehydroepiandrosterone-sulfate) is also involved in up to 40% of cases. • Sex hormone binding globulin (SHBG) levels are reduced This result in an increase in unbound (and therefore active ) androgen and oestradiol levels. • Insulin – women with PCOS are hypre-insulinaemic but are insulin-resistant. ( Hyper-insulinaemia levels of SHBG) (? PC0S mechanism )
Pathogenesis : connective Tissue AndrostenedioneOestradiol Oestrone ( ov.& adrenal ) Obesity Insulin SHBGFree Oestradiol DUB FSH Granulosa cell atresia LH No LH surgeNo ovulation Theca cell hyperplasia 5 α-reductase HirsutismDHT Androgens + Virilization Free Oestradiol
High Follicular phase LH concentrations have been found to be associate with: • Poor oocytes quality • Reduced rate of fertilization • Reduced pregnancy rate • Increase incidence of miscarriage
Diagnosis of PCOS • Oligoamenorrhea or amenorrhea and subfertility. • Symptoms of androgen excess. • U /S (Adams criteria) : 1-Many follicles 8-10 2-Follicles <10mm diameter 3-Thickened white capsule 4-Hyperechogenic stroma • Biochemical :↑LH in 40% of cases (LH/FSH>2) ↑serum testosterone in 30% of cases serum prolactin in 40% of cases
Management Principals of management : • Confirm diagnosis and identify category. • Identify and manage concurrent illness. • Identify and manage patient needs. There are numerous options for successful PCO management – medical / surgical
Preprocedural Considerations • Endometrial Neoplasia • Insulin Resistance • Metabolic Syndrome • Weight loss
Endometrial Neoplasia • Chronic anovulation associated with PCOS may lead to endometrial hyperplasia and sometimes to frank endometrial cancer (Meier and Schenker,1996). • Endometrial biopsy is indicated in all women with H/O long term unopposed estrogen exposure and in those where endometrial thickness isgreater than 12mm.
Insulin Resistance (IR) • IR is defined as reduced glucose response to a given amount of insulin. • It occurs in 80% of obese women and 30 to40% of women with normal wt. with PCOS . • Peripheral target tissue insulin resistance can be due to decreased no of peripheral insulin receptors, decreased insulin binding or a post receptor failure. • In PCOS it is caused by the post receptor defect due to excessive serine phosphorylation of beta chain of insulin receptor and of adrenal and ovarian cytochrome P450c enzyme . This enzyme is a rate limiting step in androgen biosynthesis thus leading to hyperandrogenemia .
Diagnostic criteria for metabolic syndrome Diagnosis is made when 3 or more of these risk criteria are met : • ↑ Glucose ≥ 6.1 mmol/l • Waist circumference ≥ 88 cm. • ↓ HDL-C≤ 1.3 mmol/l • ↑BP ≥ 130 / ≥ 85 mm Hg • ↑TG ≥ 1.7 mmol/l (Shroff et al.,2007)
Weight Loss • Weight loss has advantage of being effective and cheap with no side effects and should be the first line of treatment . • Weight loss improves endocrine profile and ovulation and subsequent healthy pregnancy (decreasing insulin and androgens and increasing SHBG ). • Weight loss has been shown to improve the outcome of all forms of infertility treatments, including IVF (Clark et al.,1998).
Various treatment modalities Pharmacological Treatment CC GonadotropinHyperinsulinemia? hMG Insulin sensitizer uFSH GnRH-analogs HP-FSH rec-FSH
A. Medical Treatment • Infertility is treated by increasing the rate of ovulation, in part by reducing insulin drive through exercise and weight loss . • Ovarian stimulation is used for those patients who do not ovulate, despite loosing weight by different drugs and different protocols.
Medical Treatment (cont.) • Treat Hyperprolactinaemia with Bromocriptine. • Glucocorticoids for adrenal hyperplasia . ( 0.25mg Dexamethasone at night ) • COC pills or POP for dysfunctional uterine bleeding and to reduce the risk of endometrial carcinoma .
Insulin sensitizing drugs Metformin • Action : -inhibit hepatic glucose production. -enhance sensitivity of peripheral tissues to insulin -↓ insulin secretion. • Ovarian hyperstimulation in gonadotrophin therapy • RCT- clomiphene -resistant pts., use of metformin & CC produced significant improvement
B. Surgical treatment modalities Surgical Treatment Cauterization Wedge resection ( laser, electric )
Methods of Ovarian Surgery For Ovulation Induction In PCOS • Laparoscopic Techniques of Ovarian Surgery (LOS) Laparoscopic Ovarian Drilling (LOD) : Diathermy / LASER. • Transvaginal Techniques of Ovarian Surgery (TVOS) 1) Transvaginal mini-laparoscopy (Fertiloscopy) 2) Transvaginal ultrasound (TVS)-guided ovarian drilling.
Indications I. Ovulation induction: in the following cases: a) C.C resistant PCO: Defined as failure to ovulate on a dose of 100 mg, for 5 days (recently in 3 cycles, in contrast to 6 cycles in the past ) or failure to ovulate on incremental doses of CC(50-150mg). b) C.C failure PCO: Defined whenpregnancy does not occur despite of regular ovulation on C.C for 6-9 cycles. c) C.C pregnancy failure: Defined asfailure to maintain pregnancy conceived with C.C.
Indications( cont.) II. Other potential indications: 1.LH hypersecretion. 2. Patient cannot follow treatment regularly. • Prevention of long term morbidity in PCOS patient. 4. Menstrual irregularity in PCOS patient. 5. Acne and hirsutism resistant to treatment in PCOS patient.
Mechanism of action Of LOS 1.Drainage of atretic follicles with high (Androgen+ inhibin) content. 2.Destruction of ovarian stroma that produce androgen. 3.LOS → Postoperative ↑ of FSH →↑Intra-follicular aromatase activity 1,2,3→ ↓Intra-follicular androgenic environment → remove intraovarian block to follicular maturation that precedes ovulation.
Mechanism of action Of LOS (CONT.) 4.Surgical trauma to the ovary : • Production of non steroidal factors → Restore hypothalamo-pitutary-ovarian function. • Production of ovarian growth factors{IGF-1}→ Sensitize ovary to circulating FSH.
Risks: 1-Adhesion formation, 2-Potential surgical risks (bleeding and infection) 3-Anesthesia risks, 4-Premature ovarian failure (theoretical complication)
Technique Of LOS Utero-ovarian ligament is grasped by atrumatic forceps moving the ovary (towards anterior abdominal wall& in front of the uterus).
LASER versus electrocautery for LOS: Electrocautery IS superiorwhy? 1) Less coast &easy application. 2) Achieve higher ovulation and pregnancy rate. 3) Less surface injury than CO2 LASER → Surface adhesion. 4} Effect of diathermy may last longer than the effect of LASER .
Results • Short term results: • In responders ovulation occur within 2-4 wk,& menstruation within 4-6 wks. • Ovulation rate: 50-90%.(Patient with high LH level respond better to LOS). • Cumulative Pregnancy &Live birth rates:76%-64% respectively. • Long term results: Improvement in reproductive performance is sustained for many years. (49% Of women conceived within the 1st year after LOS)
Conclusions • Obesity plays a central role in development of PCOS leading to Hyperinsulinemia in susceptible individuals. This Hyperinsulinemia may alter androgen metabolism via a variety of mechanisms, the net result of which Hyperandrogenism.
Conclusions • The management of patients with PCOS depends upon the individual patient’s complaints. • Hyperandrogenism is optimally dealt with by reducing insulin drive to the ovary, such as exercise and reducing diet
Hirsutism Definition Excessive and inappropriate growth of facial and body hair .
Causes • Endocrine- PCOS; adrenal hyperplasia/Cushing's syndrome; hypothyroidism; acromegaly . • Androgen-secreting tumours of adrenal or ovary . • Drugs- phenytoin , diazoxide , danazol , corticosteroids . • Idiopathic .
Investigation 1. Check serum testosterone – if < 5 nmol /l no further investigation .If > 5 nmol/l repeat and check urinary steroids in 24 hour sample. 2. Check serum LH and FSH . An elevated LH suggests PCOS . 3. Pelvic ultrasound will demonstrate polycystic ovaries. 4. Check thyroid function .
5. Measure serum 17-hydroxyprogesterone if congenital adrenal hyperplasia is suspected . If levels are high consider ACTH stimulation and dexamethasone suppression tests . 6. If urinary cortisol is elevated investigate for Cushing's syndrome . 7. If adrenal tumor is suspected carry out CT scans and consider direct catherisation of adrenal veins or surgical exploration .
Treatment This will depend on the cause. Sympathetic handling and reassurance are necessary at all times.
1. Polycystic ovary syndrome Induce ovulation if infertility is also a problem. combined oesrogen/progestogen pill to suppress androgen production. Response to treatment is slow at best. It may be 6 months to a year before any reduction in hirsutism is seen. Cyproterone acetate is an anti-androgen with progestogenic activity. Pregnancy must be avoided during its use. It is therefore best used cyclically (day 5-15) in combination with ethinyl Oestradiol (day 5-26) which not only helps to inhibit ovulation but also increases SHBG concentrations. This lowers the levels of free androgens.
2. Adrenal hyperplasia This is the only situation in which corticosteroid treatment – remove after localisation. 3. Androgen – producing tumours Remove after localisation. 4. Idiopathic hirsutism This may be due to end – organ hypersensitivity. There may be some response to the oesrogen/progestogen pill or spironolactone and electrolysis is useful cosmetically.