Download
1 / 1
10 likes | 142 Views
Improving Mental Health and Substance Abuse Treatment in VA Primary Care Clinics: The Behavioral Health Laboratory. J. Ross 1,2 , E. Ingram 1 , C. Beswick 1 , S. Sayers 1,2, , J Seppelt 1,2 , J. Murphy 1,2 , I. R Katz 1,2 , V. Kane 1, D. W. Oslin 1,2.

E N D
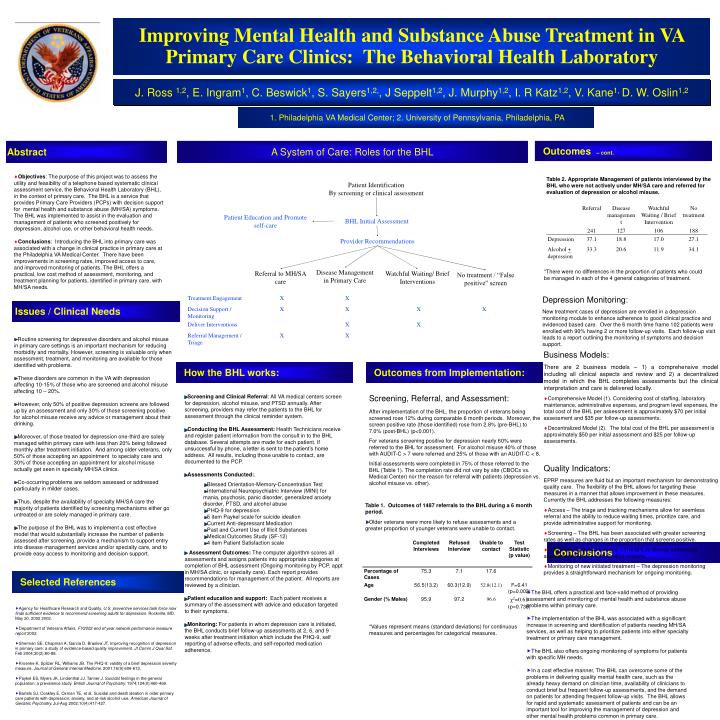
Improving Mental Health and Substance Abuse Treatment in VA Primary Care Clinics: The Behavioral Health Laboratory J. Ross 1,2, E. Ingram1, C. Beswick1, S. Sayers1,2,, J Seppelt1,2, J. Murphy1,2, I. R Katz1,2, V. Kane1, D. W. Oslin1,2 1. Philadelphia VA Medical Center; 2. University of Pennsylvania, Philadelphia, PA Abstract A System of Care: Roles for the BHL Outcomes – cont. Objectives: The purpose of this project was to assess the utility and feasibility of a telephone based systematic clinical assessment service, the Behavioral Health Laboratory (BHL), in the context of primary care. The BHL is a service that provides Primary Care Providers (PCPs) with decision support for mental health and substance abuse (MH/SA) symptoms. The BHL was implemented to assist in the evaluation and management of patients who screened positively for depression, alcohol use, or other behavioral health needs. Conclusions: Introducing the BHL into primary care was associated with a change in clinical practice in primary care at the Philadelphia VA Medical Center. There have been improvements in screening rates, improved access to care, and improved monitoring of patients. The BHL offers a practical, low cost method of assessment, monitoring, and treatment planning for patients, identified in primary care, with MH/SA needs. Table 2.Appropriate Management of patients interviewed by the BHL who were not actively under MH/SA care and referred for evaluation of depression or alcohol misuse. Patient Identification By screening or clinical assessment Patient Education and Promote self-care BHL Initial Assessment Provider Recommendations Disease Management in Primary Care *There were no differences in the proportion of patients who could be managed in each of the 4 general categories of treatment. Referral to MH/SA care Watchful Waiting/ Brief Interventions No treatment / “False positive” screen Depression Monitoring: New treatment cases of depression are enrolled in a depression monitoring module to enhance adherence to good clinical practice and evidenced based care. Over the 6 month time frame 102 patients were enrolled with 90% having 2 or more follow-up visits. Each follow-up visit leads to a report outlining the monitoring of symptoms and decision support. Issues / Clinical Needs Routine screening for depressive disorders and alcohol misuse in primary care settings is an important mechanism for reducing morbidity and mortality. However, screening is valuable only when assessment, treatment, and monitoring are available for those identified with problems. These disorders are common in the VA with depression affecting 10-15% of those who are screened and alcohol misuse affecting 10 – 20%. However, only 50% of positive depression screens are followed up by an assessment and only 30% of those screening positive for alcohol misuse receive any advice or management about their drinking. Moreover, of those treated for depression one-third are solely managed within primary care with less than 20% being followed monthly after treatment initiation. And among older veterans, only 50% of those accepting an appointment to specialty care and 30% of those accepting an appointment for alcohol misuse actually get seen in specialty MH/SA clinics. Co-occurring problems are seldom assessed or addressed particularly in milder cases. Thus, despite the availability of specialty MH/SA care the majority of patients identified by screening mechanisms either go untreated or are solely managed in primary care. The purpose of the BHL was to implement a cost effective model that would substantially increase the number of patients assessed after screening, provide a mechanism to support entry into disease management services and/or specialty care, and to provide easy access to monitoring and decision support. Business Models: There are 2 business models – 1) a comprehensive model including all clinical aspects and review and 2) a decentralized model in which the BHL completes assessments but the clinical interpretation and care is delivered locally. Comprehensive Model (1). Considering cost of staffing, laboratory maintenance, administrative expenses, and program level expenses, the total cost of the BHL per assessment is approximately $70 per initial assessment and $35 per follow-up assessments. Decentralized Model (2). The total cost of the BHL per assessment is approximately $50 per initial assessment and $25 per follow-up assessments. How the BHL works: Outcomes from Implementation: • Screening and Clinical Referral: All VA medical centers screen for depression, alcohol misuse, and PTSD annually. After screening, providers may refer the patients to the BHL for assessment through the clinical reminder system. • Conducting the BHL Assessment: Health Technicians receive and register patient information from the consult in to the BHL database. Several attempts are made for each patient. If unsuccessful by phone, a letter is sent to the patient’s home address. All results, including those unable to contact, are documented to the PCP. • Assessments Conducted:. • Blessed Orientation-Memory-Concentration Test • International Neuropsychiatric Interview (MINI) for mania, psychosis, panic disorder, generalized anxiety disorder, PTSD, and alcohol abuse • PHQ-9 for depression • 5 item Paykel scale for suicide ideation • Current Anti-depressant Medication • Past and Current Use of Illicit Substances • Medical Outcomes Study (SF-12) • 4 item Patient Satisfaction scale • Assessment Outcomes: The computer algorithm scores all assessments and assigns patients into appropriate categories at completion of BHL assessment (Ongoing monitoring by PCP, appt in MH/SA clinic, or specialty care). Each report provides recommendations for management of the patient. All reports are reviewed by a clinician. • Patient education and support: Each patient receives a summary of the assessment with advice and education targeted to their symptoms. • Monitoring: For patients in whom depression care is initiated, the BHL conducts brief follow-up assessments at 2, 6, and 9 weeks after treatment initiation which include the PHQ-9, self reporting of adverse effects, and self-reported medication adherence. Screening, Referral, and Assessment: After implementation of the BHL, the proportion of veterans being screened rose 12% during comparable 6 month periods. Moreover, the screen positive rate (those identified) rose from 2.8% (pre-BHL) to 7.0% (post-BHL) (p<0.001). For veterans screening positive for depression nearly 60% were referred to the BHL for assessment. For alcohol misuse 40% of those with AUDIT-C > 7 were referred and 25% of those with an AUDIT-C < 8. Initial assessments were completed in 75% of those referred to the BHL (Table 1). The completion rate did not vary by site (CBOCs vs. Medical Center) nor the reason for referral with patients (depression vs. alcohol misuse vs. other). Quality Indicators: EPRP measures are fluid but an important mechanism for demonstrating quality care. The flexibility of the BHL allows for targeting these measures in a manner that allows improvement in these measures. Currently the BHL addresses the following measures: Access – The triage and tracking mechanisms allow for seemless referral and the ability to reduce waiting times, prioritize care, and provide administrative support for monitoring. Screening – The BHL has been associated with greater screening rates as well as changes in the proportion that screens positive. Follow-up of positive screens – The BHL is directly addressing assessment of those with positive screens. Monitoring of new initiated treatment – The depression monitoring provides a straightforward mechanism for ongoing monitoring. Table 1.Outcomes of 1487 referrals to the BHL during a 6 month period. Older veterans were more likely to refuse assessments and a greater proportion of younger veterans were unable to contact. Conclusions Selected References • The BHL offers a practical and face-valid method of providing assessment and monitoring of mental health and substance abuse problems within primary care. • The implementation of the BHL was associated with a significant increase in screening and identification of patients needing MH/SA services, as well as helping to prioritize patients into either specialty treatment or primary care management. • The BHL also offers ongoing monitoring of symptoms for patients with specific MH needs. • In a cost effective manner, The BHL can overcome some of the problems in delivering quality mental health care, such as the already heavy demand on clinician time, availability of clinicians to conduct brief but frequent follow-up assessments, and the demand on patients for attending frequent follow-up visits. The BHL allows for rapid and systematic assessment of patients and can be an important tool for improving the management of depression and other mental health problems common in primary care. • Agency for Healthcare Research and Quality. U.S. preventive services task force now finds sufficient evidence to recommend screening adults for depression. Rockville, MD. May 20, 2002 2002. • Department of Veterans Affairs. FY2002 end of year network performance measure report 2002. • Sherman SE, Chapman A, Garcia D, Braslow JT. Improving recognition of depression in primary care: a study of evidence-based quality improvement. Jt Comm J Qual Saf. Feb 2004;30(2):80-88. • Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. Journal of General Internal Medicine. 2001;16(9):606-613. • Paykel ES, Myers JK, Lindenthal JJ, Tanner J. Suicidal feelings in the general population: a prevalence study. British Journal of Psychiatry. 1974;124(0):460-469. • Bartels SJ, Coakley E, Oxman TE, et al. Suicidal and death ideation in older primary care patients with depression, anxiety, and at-risk alcohol use. American Journal of Geriatric Psychiatry. Jul-Aug 2002;10(4):417-427. *Values represent means (standard deviations) for continuous measures and percentages for categorical measures.



















