Download
1 / 1
10 likes | 176 Views
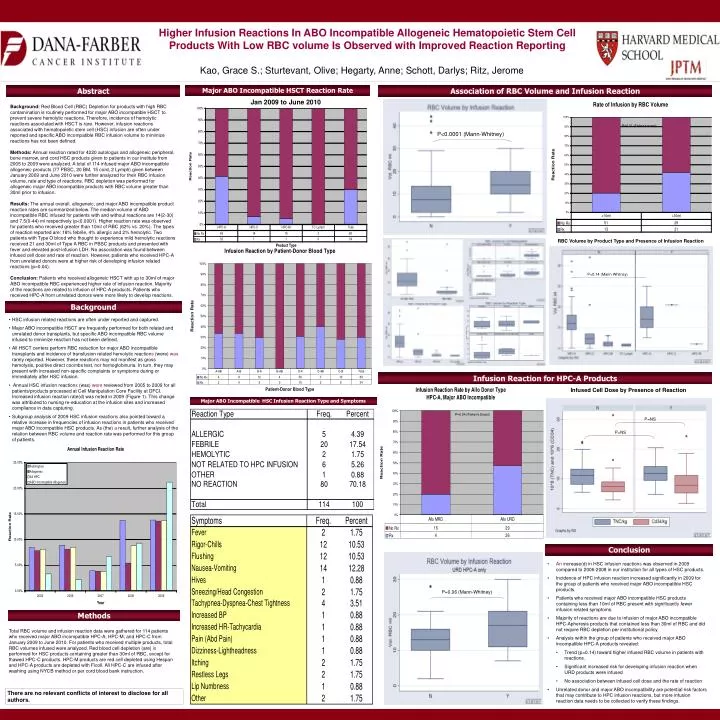
Jan 2009 to June 2010. P<0.0001 (Mann-Whitney). RBC Volume by Product Type and Presence of Infusion Reaction. P=0.14 (Mann-Whitney). Infused Cell Dose by Presence of Reaction. P=NS. P=0.04 (Fisher’s Exact). P=NS. P=0.06 (Mann-Whitney).

E N D
Jan 2009 to June 2010 P<0.0001 (Mann-Whitney) RBC Volume by Product Type and Presence of Infusion Reaction P=0.14 (Mann-Whitney) Infused Cell Dose by Presence of Reaction P=NS P=0.04 (Fisher’s Exact) P=NS P=0.06 (Mann-Whitney) Higher Infusion Reactions In ABO Incompatible Allogeneic Hematopoietic Stem Cell Products With Low RBC volume Is Observed with Improved Reaction Reporting Kao, Grace S.; Sturtevant, Olive; Hegarty, Anne; Schott, Darlys; Ritz, Jerome Abstract Association of RBC Volume and Infusion Reaction Major ABO Incompatible HSCT Reaction Rate Background: Red Blood Cell (RBC) Depletion for products with high RBC contamination is routinely performed for major ABO incompatible HSCT to prevent severe hemolytic reactions. Therefore, incidence of hemolytic reactions associated with HSCT is rare. However, infusion reactions associated with hematopoietic stem cell (HSC) infusion are often under reported and specific ABO incompatible RBC infusion volume to minimize reactions has not been defined. Methods: Annual reaction rated for 4220 autologus and allogeneic peripheral, bone marrow, and cord HSC products given to patients in our institute from 2005 to 2009 were analyzed. A total of 114 infused major ABO incompatible allogeneic products (77 PBSC, 20 BM, 15 cord, 2 Lymph) given between January 2009 and June 2010 were further analyzed for their RBC infusion volume, rate and type of reactions. RBC depletion was performed for allogeneic major ABO incompatible products with RBC volume greater than 30ml prior to infusion. Results: The annual overall, allogeneic, and major ABO incompatible product reaction rates are summarized below. The median volume of ABO incompatible RBC infused for patients with and without reactions are 14(2-30) and 7.5(0-44) ml respectively (p<0.0001). Higher reaction rate was observed for patients who received greater than 10ml of RBC (62% vs. 20%). The types of reaction reported are: 18% febrile, 4% allergic and 2% hemolytic. Two patients with Type O blood who thought to experience mild hemolytic reactions received 21 and 30ml of Type A RBC in PBSC products and presented with fever and elevated post-infusion LDH. No association was found between infused cell dose and rate of reaction. However, patients who received HPC-A from unrelated donors were at higher risk of developing infusion related reactions (p=0.04). Conclusion: Patients who received allogeneic HSCT with up to 30ml of major ABO incompatible RBC experienced higher rate of infusion reaction. Majority of the reactions are related to infusion of HPC-A products. Patients who received HPC-A from unrelated donors were more likely to develop reactions. P=0.01 (Fisher’s exact) Background • HSC infusion related reactions are often under reported and captured. • Major ABO incompatible HSCT are frequently performed for both related and unrelated donor transplants, but specific ABO incompatible RBC volume infused to minimize reaction has not been defined. • All HSCT centers perform RBC reduction for major ABO incompatible transplants and incidence of transfusion related hemolytic reactions (were) was rarely reported. However, these reactions may not manifest as gross hemolysis, positive direct coombs test, nor hemoglobinuria. In turn, they may present with increased non-specific complaints or symptoms during or immediately after HSC infusion. • Annual HSC infusion reactions (was) were reviewed from 2005 to 2009 for all patients/products processed at Cell Manipulation Core Facility at DFCI. Increased infusion reaction rate(d) was noted in 2009 (Figure 1). This change was attributed to nursing re-education at the infusion sites and increased compliance in data capturing. • Subgroup analysis of 2009 HSC infusion reactions also pointed toward a relative increase in frequencies of infusion reactions in patients who received major ABO incompatible HSC products. As (the) a result, further analysis of the relation between RBC volume and reaction rate was performed for this group of patients. Infusion Reaction for HPC-A Products Major ABO Incompatible HSC Infusion Reaction Type and Symptoms Conclusion • An increase(d) in HSC infusion reactions was observed in 2009 compared to 2006-2008 in our institution for all types of HSC products. • Incidence of HPC infusion reaction increased significantly in 2009 for the group of patients who received major ABO incompatible HSC products. • Patients who received major ABO incompatible HSC products containing less than 10ml of RBC present with significantly fewer infusion related symptoms. • Majority of reactions are due to infusion of major ABO incompatible HPC-Apheresis products that contained less than 30ml of RBC and did not require RBC depletion per institutional policy. • Analysis within the group of patients who received major ABO incompatible HPC-A products revealed: • Trend (p=0.14) toward higher infused RBC volume in patients with reactions. • Significant increased risk for developing infusion reaction when URD products were infused • No association between infused cell dose and the rate of reaction • Unrelated donor and major ABO incompatibility are potential risk factors that may contribute to HPC infusion reactions, but more infusion reaction data needs to be collected to verify these findings. Methods Total RBC volume and infusion reaction data were gathered for 114 patients who received major ABO incompatible HPC-A, HPC-M, and HPC-C from January 2009 to June 2010. For patients who received multiple products, total RBC volumes infused were analyzed. Red blood cell depletion (are) is performed for HSC products containing greater than 30ml of RBC, except for thawed HPC-C products. HPC-M products are red cell depleted using Hespan and HPC-A products are depleted with Ficoll. All HPC-C are infused after washing using NYCB method or per cord blood bank instruction. There are no relevant conflicts of interest to disclose for all authors.



















